A Patient’s Guide to Stress Fracture of the Hip
Introduction
Stress fractures of the hip once most commonly affected military personnel who marched and ran day after day. Today, stress fractures of the hip are more common in athletes, especially distance runners.
There are two types of stress fractures. Insufficiency fractures are breaks in abnormal bone under normal force. Fatigue fractures are breaks in normal bone that has been put under extreme force. Fatigue fractures are usually caused by new, strenuous, very repetitive activities, such as marching or distance running. Most stress fractures of the hip are fatigue fractures. The stress fractures this article refers to are fatigue fractures.
This guide will help you understand
- how a stress fracture develops
- how doctors diagnose the condition
- what treatment options are available
Anatomy
What is a stress fracture, and what part of the hip is involved?
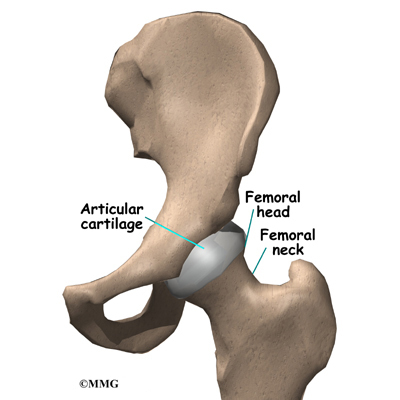
The femur is the large bone in the thigh. The ball-shaped head of the femur fits into a socket in the pelvis, called the acetabulum. When a stress fracture occurs in the hip, it usually involves the femoral neck, the short section of bone that connects the head of the femur to the main shaft of the bone. The femoral neck is a thinner part of the femur. Stress fractures are hairline cracks in the bone that can grow larger over time if not treated properly.
The femoral neck has to withstand extreme force even during normal activities, such as standing still. The normal contraction of muscles during walking makes this stress even higher. Running triples the stress on the femoral neck.
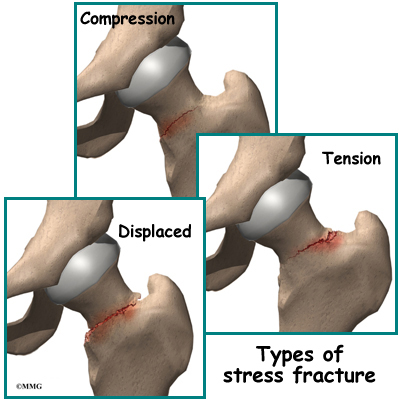
Surgeons put fatigue fractures of the femoral neck into three categories. Compression fractures occur on the underside of the femoral neck. Tension fractures occur on the upper side of the bone and can cause more problems than fractures on the underside of the femoral neck. In displaced fractures, the bone cracks all the way through, and the two bones no longer line up correctly.
A displaced stress fracture is a very serious problem in a young adult because it may lead to damage to the blood vessels going into the upper end of the hip bone. This can cause a very serious complication known as avascular necrosis (AVN) of the hip.
Related Document: A Patient’s Guide to Avascular Necrosis of the Hip
Patients with fatigue stress fractures of the hip are also likely to have muscle and tendon injuries and swelling of the synovial lining (the lubricated lining) of the hip joint.
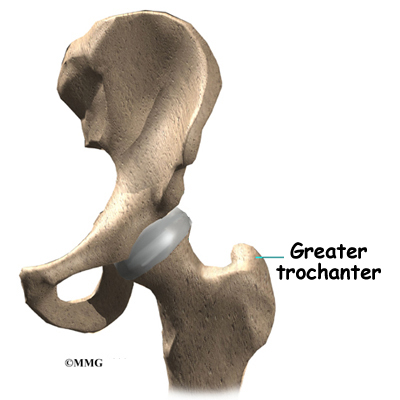
Stress fractures can also happen in the shaft of the femur bone, the greater trochanter, and the pelvis bone. The greater trochanter is a large bump below the neck of the femur. The buttock muscles that move the hip connect to this part of the femur.
Related Document: A Patient’s Guide to Hip Anatomy
Causes
Why do I have this problem?
Doctors think that putting extreme stress on the bone over and over again causes stress fractures of the hip. Think of how you can break a metal paper clip by bending it back and forth repeatedly.
Bones can usually adapt to repetitive stress, and any change in the function of a bone causes it to change the way it is built. This is how small bumps and ridges form on bones. The tendons pull on these areas, and the bone adapts by building up. This is normal. But extreme stress repeated too often can overwhelm the bone’s ability to adapt. This is especially true when someone suddenly begins a new, strenuous, repetitive activity such as running.
Fatigue fractures are related to both the amount of exercise and how fast people increase their exercise program. The more people run or march, the more likely they are to develop a fatigue fracture. Research suggests that most athletes who develop stress fractures have been training for at least two years, six or more times a week. A stress fracture is more likely to occur after an increase in how far, how often, and how hard a person goes.
Women are up to 10 times more likely to develop fatigue fractures than men. The reasons for this are unclear. Hormonal changes may make women athletes’ bones more likely to fracture. Eating disorders, which are more common in women athletes, may also make bones more likely to fracture.
Age also makes stress fractures of the hip more likely. This is thought to be due to declining levels of physical fitness more than age.
Symptoms
What does a stress fracture of the hip feel like?
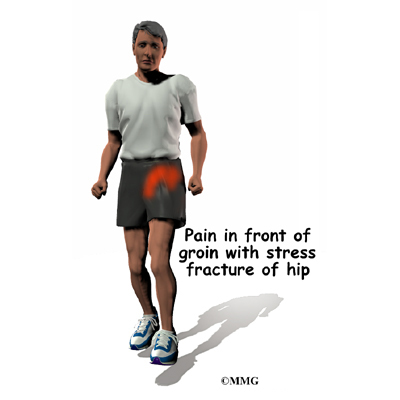
Most patients with stress fractures of the hip feel pain in the front of the groin while standing and moving. Rest usually makes the pain go away. Patients may limp. Strenuous activities, such as running and climbing stairs, may be so painful that the patient must stop doing them.
Diagnosis
How do doctors identify the condition?
Your doctor will take a detailed medical history and ask many questions about your activities and exercise. Your doctor will also physically examine the painful hip. One of your doctor’s main goals will be to determine if other problems, such as muscle or tendon injuries, are causing some or all of your pain.
Your doctor will probably suggest taking an X-ray of your hip. The X-ray may help rule out other problems, but it probably will not show the stress fracture.
Your doctor may recommend other imaging tests that are more likely to show a stress fracture. A bone scan may be suggested to look for early signs of a stress fracture. A bone scan involves injecting tracers into your blood stream. The tracers then show up on special X-rays of your hip. The tracers build up in areas of extra strain to bone tissue, such as a stress fracture.
The magnetic resonance imaging (MRI) scan is especially useful in telling fatigue fractures from other types of injuries with similar symptoms. The MRI is being used increasingly in cases where doctors suspect a stress fracture.
Treatment
What can be done for the problem?
The treatment your doctor recommends will depend on the type of fracture you have.
Nonsurgical Treatment
Doctors most often recommend nonsurgical treatment for compression-type fatigue fractures. You must stay off the affected leg, using crutches if necessary, and rest the hip for at least four to six weeks. Pain can be treated with hot and cold treatments and medication. With care, the fractures tend to heal by themselves.
Surgeons do not all agree on how to treat tension fractures. If the fracture is not at risk for displacing, surgeons may have patients use crutches to keep strain off the hip during standing and walking. X-rays are taken every few weeks to make sure the bone is healing. If the tension fracture is in danger of displacing, however, most surgeons will operate. This is because the complication of AVN can cause the femoral head to actually lose its blood supply and collapse. This leads very rapidly to degenerative arthritis of the hip joint. Because these effects can be so devastating, most surgeons recommend surgery if they feel that the stress fracture is in danger of displacing.
Surgery
In some patients with a fracture under the femoral neck, MRIs and other imaging tests sometimes show an unstable fracture that needs to be surgically fixed.
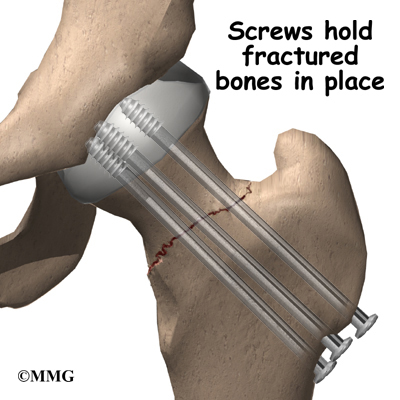
The surgical procedure is the same whether the stress fracture is stable or there is only a slight displacement of the bones. If your surgeon recommends surgery for a stress fracture of the hip, several large metal screws will be inserted through the femoral neck to hold the fractured bones in place while the fracture heals.
To perform this procedure, a small incision is made on the side of the upper thigh. With the help of a special X-ray machine called a fluoroscope, the surgeon can insert the metal screws into the proper position while watching the X-ray image on a TV screen.
When the ends of the bones show a large displacement, surgeons aren’t in total agreement about which surgery is best. Most surgeons agree that younger, active patients benefit if surgery is done to save the femoral head. This method also uses screws to connect the two sections of bone.
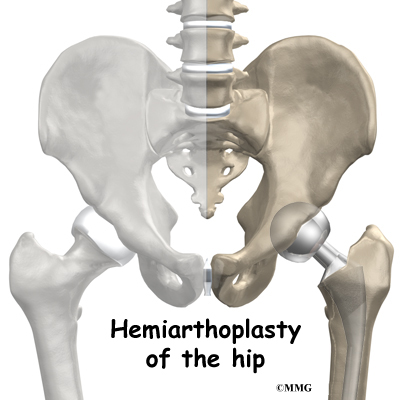
To avoid problems with AVN, other surgeons feel that older, less active patients should have part or all of the hip joint replaced. If the socket of the joint is healthy, the surgeon may decide to replace only the ball portion of the joint, a procedure called hemiarthroplasty.
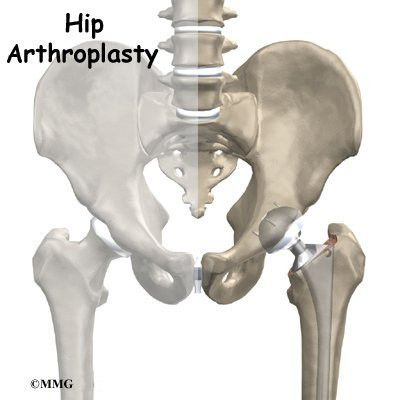
The procedure to replace both the ball and the socket with an artificial joint is called total hip arthroplasty.
Related Document: A Patient’s Guide to Hemiarthroplasty of the Hip
Related Document: A Patient’s Guide to Artificial Joint Replacement of the Hip
Rehabilitation
What should I expect following treatment?
Nonsurgical Rehabilitation
Treating a stress fracture without surgery requires patients to strictly avoid putting weight down on the foot of the injured leg when they are standing or walking. Some surgeons allow their patients to use crutches and touch only their toes down on the injured side. Others prefer that their patients rely on crutches to completely avoid putting any weight down.
Your surgeon will probably have X-rays taken every few weeks to make sure the bones are lined up and healing. When your surgeon sees that the bones are healing, you’ll be able to put more weight on your foot as you stand and walk. A physical therapist may direct your rehabilitation to help you improve strength and flexibility in the hip and to make sure you are able to safely resume your activities.
After Surgery
Recovery after surgery for hip fracture depends on the type of procedure used. The aim of most surgical procedures for a fractured hip is to help people get moving and walking as quickly as possible. This helps them avoid dangerous complications that can happen from being immobilized, such as pneumonia, blood clots, joint stiffness, and pain.
A physical therapist may work with you in the hospital soon after surgery. Treatments are used to help you begin walking with crutches or a walker, to help you access the bathroom, and to gradually improve your hip motion and strength.
During your recovery, you should follow your surgeon’s instructions about how much weight you can put down while standing or walking.
After you return home from the hospital, your surgeon may have you work with a physical therapist for two to four in-home visits. These visits are to ensure you are safe in and about the home and getting in and out of a car. Your therapist will make recommendations about your safety, review your hip precautions, and make sure you are placing a safe amount of weight on your foot when standing or walking. Home therapy visits end when you are safe to get out of the house.
A few additional visits in outpatient physical therapy may be needed for patients who are still having problems walking or who need to get back to physically heavy work or activities.
The therapist’s goal is to help you maximize hip strength, restore a normal walking pattern, and help you do your activities without risking further injury to your hip. When you are well under way, regular visits to the therapist’s office will end. Your therapist will continue to be a resource, but you will be in charge of doing your exercises as part of an ongoing home program.