We use our hands constantly, placing them in harm’s way continuously. Injuries to the finger joints are common and usually heal without significant problems. Some injuries are more serious and may develop problems if not treated carefully. One such injury is a sprain of the proximal interphalangeal joint, or PIP joint, of the finger. This joint is one of the most unforgiving joints in the body to injury. What appears at first to be a simple sprain of the PIP joint may result in a painful and stiff finger, making it difficult to use the hand for gripping activities.
This guide will help you understand
What parts of the finger are involved?
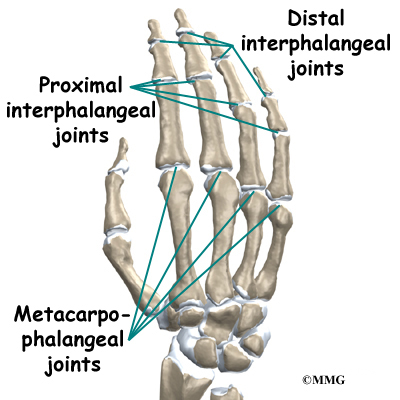
The finger joints work like hinges when the fingers bend and straighten. The main knuckle joint is the metacarpophalangeal joint (MCP joint). It is formed by the connection of the metacarpal bone in the palm of the hand with the finger bone, or phalange. Each finger has three phalanges, separated by two interphalangeal joints (IP joints). The one closest to the MCP joint (knuckle) is called the proximal IP joint (PIP joint). The joint near the end of the finger is called the distal IP joint (DIP joint).
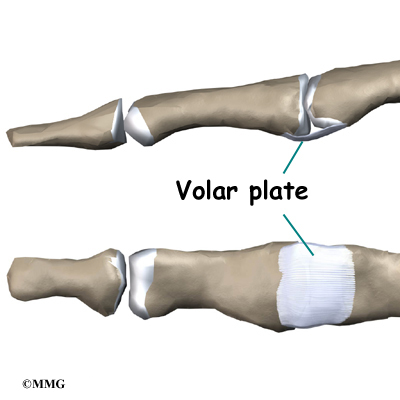
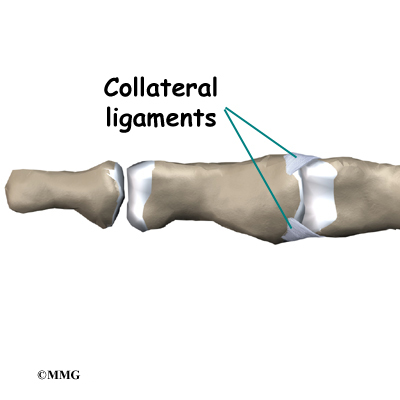
Ligaments are tough bands of tissue that connect bones together. Several ligaments hold the joints together. In the PIP joint, the strongest ligament is the volar plate. This ligament connects the proximal phalanx to the middle phalanx on the palm side of the joint. The ligament tightens as the joint is straightened and keeps the joint from hyperextending. There is also a collateral ligament on each side of the PIP joint. The collateral ligaments tighten when the joint is bent sideways and keep the joint stable from side to side.
Related Document: A Patient’s Guide to Hand Anatomy
How do these injuries of the PIP joint occur?
A sprain is a general term that means a ligament is injured. Doctors usually use this term to mean that the ligament has been stretched and partially torn. If the ligament is stretched too far, it ruptures or tears completely.
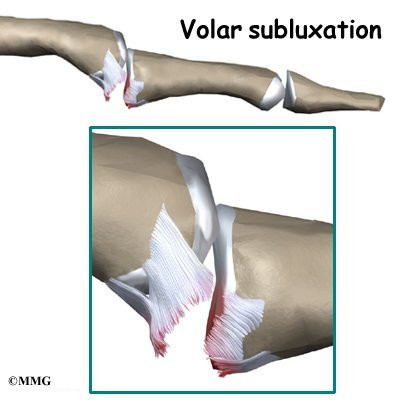
Injury to the volar plate can occur when the joint is hyperextended. If a complete tear occurs, the ligament usually ruptures or tears from its attachment on the middle phalanx. There may be a small piece of bone avulsed (pulled away) from the middle phalanx when this occurs. If it is small it is usually of no consequence, but if it is large and involves a significant amount of the joint surface it may require surgery to fix the fragment and restore the joint surface.
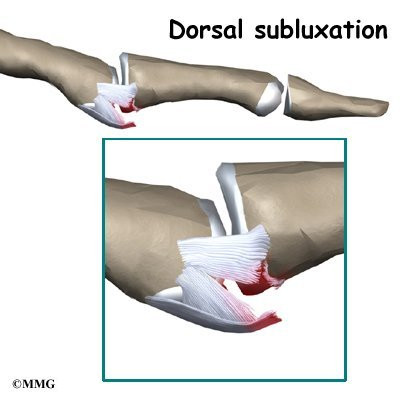
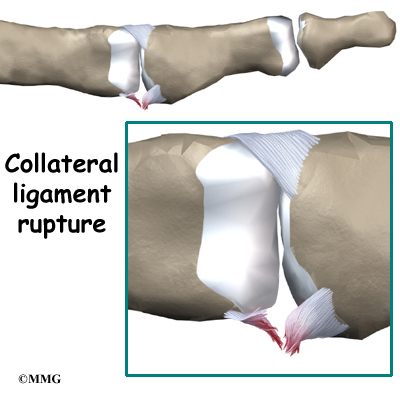
Injury to the collateral ligaments can occur when the joint is forced to bend too far sideways until one of the collateral ligaments ruptures. These ligaments can also be injured if the PIP joint is actually dislocated, with the middle phalanx dislocating behind the proximal phalanx.
What do PIP joint injuries look and feel like?
Initially, the finger is painful and swollen around the PIP joint. If the joint has completely dislocated it will appear deformed.
What tests will my doctor do?
Usually the diagnosis is evident just from the physical examination. X-rays are required to see if there is an associated avulsion fracture since this may change the recommended treatment. X-rays are also useful to see if the joint is aligned properly after an injury or after the reduction of a dislocation. No other tests are required normally.
How will my PIP joint injury be treated?
When the ligaments have been sprained or partially torn, treatment may simply consist of a short period of splinting and early exercise. The PIP joint is very sensitive to injury and becomes stiff very rapidly when immobilized for even short periods of time. The faster the joint begins to move the less likely there will be a problem with stiffness later on. Many sprains can be treated with simple buddy taping to the adjacent finger. This allows the good finger to brace to the injured finger while at the same time using the good finger to bend the injured finger as the hand is used.
When the volar plate has been completely ruptured or when the joint has been dislocated, nonsurgical treatment is still usually suggested. The goal is to keep the joint in a stable position while beginning motion as soon as possible. Since the injury results from hyperextension, a brace to prevent the joint from straightening completely while still allowing the joint to bend accomplishes both of these goals. This brace is called a dorsal blocking splint. The brace is usually worn for three to four weeks until the ligament heals enough to stabilize the joint.
In some cases when the volar plate ruptures, it may get caught in the joint and prevent the doctor from reducing (realigning) the joint without surgery.
In severe cases, surgery is necessary to repair extensive damage to the collateral ligaments or volar plate. Surgery is also necessary to remove the volar plate if it becomes trapped in the joint and prevents the surgeon from realigning the joint without surgery.
What will my recovery be like?
If nonsurgical treatment is successful, you may see improvement in three to six weeks. By wearing a dorsal blocking splint, the joint continues to bend freely but is kept from straightening completely.
After three to four weeks, the joint should heal enough to remove the splint and begin strengthening exercises. These exercises may be directed by a physical or occupational therapist.
Injuries to the PIP joint remain swollen for long periods of time. Commonly, the joint will be permanently enlarged due to the scarring of the healing process. This may cause problems with getting rings on and off. It is a good idea to wait for about one year before the ring is resized since the scarring will continue to remodel. The joint will gradually get smaller and in some cases may return to its original size.
You’ll wear a splint or brace for three weeks after surgery to give the repair time to heal. Patients may be seen for physical or occupational therapy afterward. You will likely need to attend therapy sessions for two to three months, and you should expect full recovery to take up to four months.
The first few therapy treatments will focus on controlling the pain and swelling from surgery. Then you’ll begin gentle range-of-motion exercise. Strengthening exercises are used to give added stability around the finger joint. You’ll learn ways to grip and support items in order to do your tasks safely and with the least amount of stress on your finger joint. As with any surgery, you need to avoid doing too much, too quickly.
Eventually, you’ll begin doing exercises designed to get your hand and fingers working in ways that are similar to your work tasks and daily activities. Your therapist will help you find ways to do your tasks that don’t put too much stress on your finger joint. Before your therapy sessions end, your therapist will teach you a number of ways to avoid future problems.
Your therapist’s goal is to help you keep your pain under control, improve your strength and range of motion, and regain fine motor abilities with your hand and finger. When your are well under way, regular visits to your therapist’s office will end. Your therapist will continue to be a resource, but you will be in charge of doing your exercises as part of an ongoing home program.
https://www.youtube.com/watch?v=cyXf5YbnJKs Artificial Hip Replacement Anterior Approach (Hip Arthroplasty)
https://www.youtube.com/watch?v=m8LDBlZN-XM Artificial Knee Replacement (Knee Arthroplasty) Animated Tutorial
https://www.youtube.com/watch?v=0qR-Yfw9fOI Lumbar Spine Anatomy Animated Tutorial
https://www.youtube.com/watch?v=RNUpMNd_u1U Cervical Spine Anatomy Animated Tutorial
https://www.youtube.com/watch?v=qlCvKEOZtpo Hip Anatomy Animated Tutorial
https://www.youtube.com/watch?v=_q-Jxj5sT0g Knee Anatomy Animated Tutorial
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}