The shoulder is a very complex piece of machinery. Its elegant design gives the shoulder joint great range of motion, but not much stability. As long as all the parts are in good working order, the shoulder can move freely and painlessly.
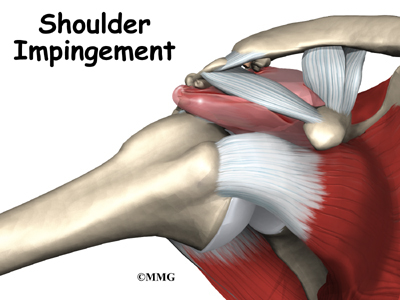
Many people refer to any pain in the shoulder as bursitis. The term bursitis really only means that the part of the shoulder called the bursa is inflamed. Tendonitis is when a tendon gets inflamed. This can be another source of pain in the shoulder. Many different problems can cause inflammation of the bursa or tendons. Impingement syndrome is one of those problems. Impingement syndrome occurs when the rotator cuff tendons rub against the roof of the shoulder, the acromion.
This guide will help you understand
What part of the shoulder is affected?
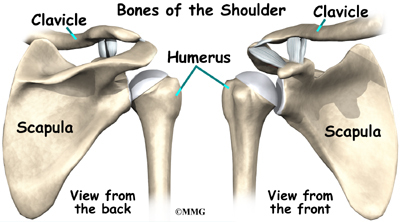
The shoulder is made up of three bones: the scapula (shoulder blade), the humerus (upper arm bone), and the clavicle (collarbone).
The rotator cuff connects the humerus to the scapula. The rotator cuff is formed by the tendons of four muscles: the supraspinatus, infraspinatus, teres minor, and subscapularis.
Tendons attach muscles to bones. Muscles move the bones by pulling on the tendons. The rotator cuff helps raise and rotate the arm.
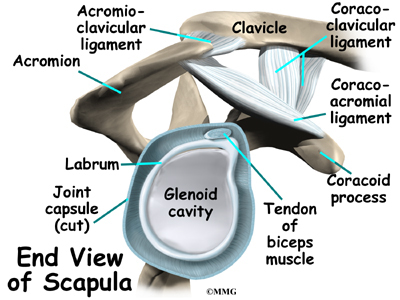
As the arm is raised, the rotator cuff also keeps the humerus tightly in the socket of the scapula, the glenoid. The upper part of the scapula that makes up the roof of the shoulder is called the acromion.
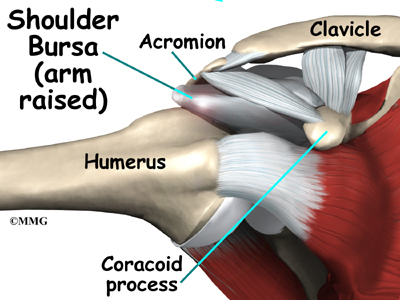
A bursa is located between the acromion and the rotator cuff tendons. A bursa is a lubricated sac of tissue that cuts down on the friction between two moving parts. Bursae are located all over the body where tissues must rub against each other. In this case, the bursa protects the acromion and the rotator cuff from grinding against each other.
Related Document: A Patient’s Guide to Shoulder Anatomy
Why do I have problems with shoulder impingement?
Usually, there is enough room between the acromion and the rotator cuff so that the tendons slide easily underneath the acromion as the arm is raised. But each time you raise your arm, there is a bit of rubbing or pinching on the tendons and the bursa. This rubbing or pinching action is called impingement.
Impingement occurs to some degree in everyone’s shoulder. Day-to-day activities that involve using the arm above shoulder level cause some impingement. Usually it doesn’t lead to any prolonged pain. But continuously working with the arms raised overhead, repeated throwing activities, or other repetitive actions of the shoulder can cause impingement to become a problem. Impingement becomes a problem when it causes irritation or damage to the rotator cuff tendons.
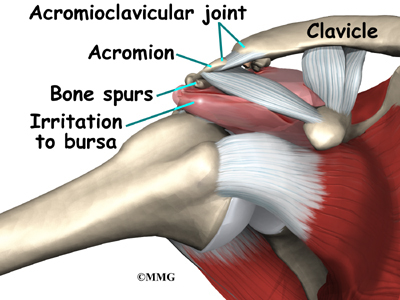
Raising the arm tends to force the humerus against the edge of the acromion. With overuse, this can cause irritation and swelling of the bursa. If any other condition decreases the amount of space between the acromion and the rotator cuff tendons, the impingement may get worse.
Bone spurs can reduce the space available for the bursa and tendons to move under the acromion. Bone spurs are bony points. They are commonly caused by wear and tear of the joint between the collarbone and the scapula, called the acromioclavicular (AC) joint. The AC joint is directly above the bursa and rotator cuff tendons.
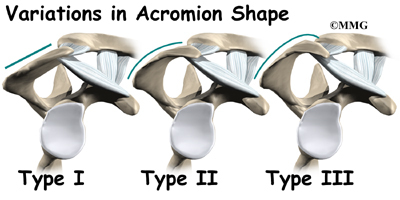
In some people, the space is too small because the acromion is oddly sized. In these people, the acromion tilts too far down, reducing the space between it and the rotator cuff.
What does impingement syndrome feel like?
Impingement syndrome causes generalized shoulder aches in the condition’s early stages. It also causes pain when raising the arm out to the side or in front of the body. Most patients complain that the pain makes it difficult for them to sleep, especially when they roll onto the affected shoulder.
A reliable sign of impingement syndrome is a sharp pain when you try to reach into your back pocket. As the condition worsens, the discomfort increases. The joint may become stiffer. Sometimes a catching sensation is felt when you lower your arm. Weakness and inability to raise the arm may indicate that the rotator cuff tendons are actually torn.
Related Document: A Patient’s Guide to Rotator Cuff Tears
What tests will my doctor run?
The diagnosis of bursitis or tendonitis caused by impingement is usually made on the basis of your medical history and physical examination. Your doctor will ask you detailed questions about your activities and your job, because impingement is frequently related to repeated overhead activities.
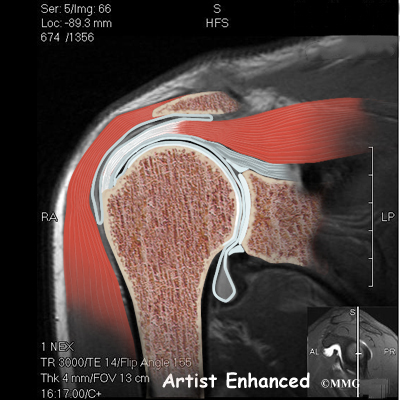
Your doctor may order X-rays to look for an abnormal acromion or bone spurs around the AC joint. A magnetic resonance imaging (MRI) scan may be performed if your doctor suspects a tear of the rotator cuff tendons. An MRI is a special imaging test that uses magnetic waves to create pictures that show the tissues of the shoulder in slices. The MRI scan shows tendons as well as bones. The MRI scan is painless and requires no needles.
An arthrogram may also be used to detect rotator cuff tears. The arthrogram is an older test than the MRI, but it is still widely used. It involves injecting dye into the shoulder joint and then taking several X-rays. If the dye leaks out of the shoulder joint, it suggests that there is a tear in the rotator cuff tendons.
In some cases, it is unclear whether the pain is coming from the shoulder or a pinched nerve in the neck. An injection of a local anesthetic (such as lidocaine) into the bursa can confirm that the pain is in fact coming from the shoulder. If the pain goes away immediately after the injection, then the bursa is the most likely source of the pain. Pain from a pinched nerve in the neck would almost certainly not go away after an injection into the shoulder.
What treatment options are available?
Doctors usually start by prescribing nonsurgical treatment. You may be prescribed anti-inflammatory medications such as aspirin or ibuprofen. Resting the sore joint and putting ice on it can also ease pain and inflammation. If the pain doesn’t go away, an injection of cortisone into the joint may help. Cortisone is a strong medication that decreases inflammation and reduces pain. Cortisone’s effects are temporary, but it can give very effective relief for up to several months.
Related Document: A Patient’s Guide to Joint Injections for Arthritis
Your doctor may also prescribe sessions with a physical or occupational therapist. Your therapist will use various treatments to calm inflammation, including heat and ice. Therapists use hands-on treatments and stretching to help restore full shoulder range of motion. Improving strength and coordination in the rotator cuff and shoulder blade muscles lets the humerus move in the socket without pinching the tendons or bursa under the acromion. You may need therapy treatments for four to six weeks before you get full shoulder motion and function back.
If you are still having problems after trying nonsurgical treatments, your doctor may recommend surgery.
Subacromial Decompression
The goal of surgery is to increase the space between the acromion and the rotator cuff tendons. Taking pressure off the tissues under the acromion is called subacromial decompression. The surgeon must first remove any bone spurs under the acromion that are rubbing on the rotator cuff tendons and the bursa. Usually the surgeon also removes a small part of the acromion to give the tendons even more space. In patients who have a downward tilt of the acromion, more of the bone may need to be removed. Surgically cutting and shaping the acromion is called acromioplasty. It gives the surgeon another step to get pressure off (decompress) the tissues between the humerus and the acromion.
Resection Arthroplasty
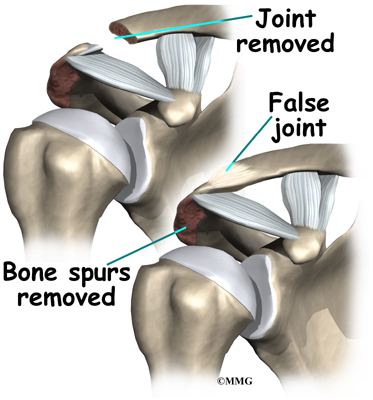
Impingement may not be the only problem in an aging or overused shoulder. It is very common to also see degeneration from arthritis in the AC joint. If there is reason to believe that the AC joint is arthritic, the end of the clavicle may be removed during impingement surgery. This procedure is called a resection arthroplasty.
The most common procedure for AC joint osteoarthritis is resection arthroplasty. A resection arthroplasty involves removing a small portion of the end of the clavicle. This leaves a space between the acromion (the piece of the scapula that meets your shoulder) and the cut end of the clavicle, where the joint used to be. Your surgeon will take care not to remove too much of the end of the clavicle to prevent any damage to the ligaments holding the joint together. Usually only a small portion is removed, less than one cm (about three-eighths of an inch). As your body heals, the joint is replaced by scar tissue. Remember, the AC joint doesn’t move much, but it does need to be flexible. The scar tissue allows movement but stops the bone ends from rubbing together.
This procedure can be done in two ways. Today, it is more common to do this procedure using the arthroscope. An arthroscope is a slender tool with a tiny TV camera on the end. It lets the surgeon work in the joint through a very small incision. This may result in less damage to the normal tissues surrounding the joint, leading to faster healing and recovery.
Related Document: A Patient’s Guide to Osteoarthritis of the Acromioclavicular Joint
Arthroscopic Procedure
Today, acromioplasty is usually done using an arthroscope.
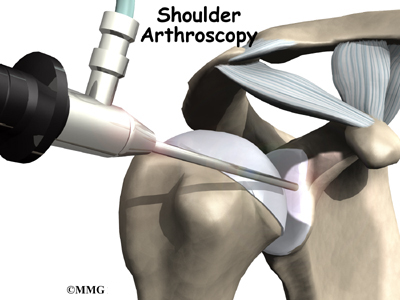
An arthroscope is a special type instrument designed to look into a joint, or other space, inside the body. The arthroscope itself is a slender metal tube smaller than a pencil. Inside the metal tube are special strands of glass called fiberoptics. These small strands of glass form a lens that allows one to look into the tube on one end and see what is on the other side – inside the space. This is similar to a microscope or telescope. In the early days of arthroscopy, the surgeon actually looked into one end of the tube. Today, the arthroscope is attached to a small TV camera. The surgeon can watch the TV screen while the arthroscope is moved around in the joint. Using the ability to see inside the joint, the surgeon can then place other instruments into the joint and perform surgery while watching what is happening on the TV screen.
The arthroscope lets the surgeon work in the joint through a very small incision. This may result in less damage to the normal tissues surrounding the joint, leading to faster healing and recovery. If your surgery is done with the arthroscope, you may be able to go home the same day.
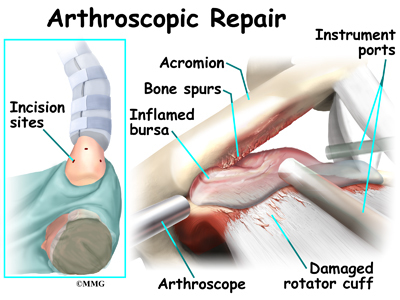
To perform the acromioplasty using the arthroscope, several small incisions are made to insert the arthroscope and special instruments needed to complete the procedure. These incisions are small, usually about one-quarter inch long. It may be necessary to make three or four incisions around the shoulder to allow the arthroscope to be moved to different locations to see different areas of the shoulder.
A small plastic, or metal, tube is inserted into the shoulder and connected with sterile plastic tubing to a special pump. Another small tube allows the fluid to be removed from the joint. This pump continuously fills the shoulder joint with sterile saline (salt water) fluid. This constant flow of fluid through the joint inflates the joint and washes any blood and debris from the joint as the surgery is performed.
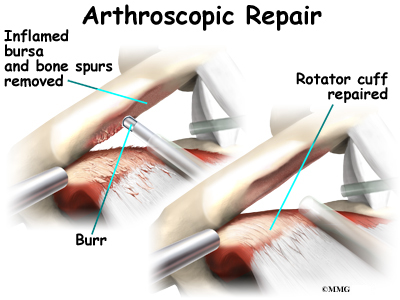
There are many small instruments that have been specially designed to perform surgery in the joint. Some of these instruments are used to remove torn and degenerative tissue. Some of these instruments nibble away bits of tissue and then vacuum them up from out of the joint. Others are designed to burr away bone tissue and vacuum it out of the joint. These instruments are used to remove any bone spurs that are rubbing on the tendons of the shoulder and smooth the under surface of the acromion and AC joint.
Open Procedure
In other cases, an open incision is made to allow removal of the bone. Usually an incision about three or four inches long is made over the top of the shoulder. The surgeon removes any bone spurs and a part of the acromion. The surgeon then smooths the rough ends of the bone. If necessary, the surgeon will do a resection arthroplasty on the AC joint. If you have open surgery, you may need to spend a night or two in the hospital.
View animation of bone spur removal
What should I expect after treatment?
Even if you don’t need surgery, you may need to follow a program of rehabilitation exercises. Your doctor may recommend that you work with a physical or occupational therapist. Your therapist can create an individualized program of strengthening and stretching for your shoulder and rotator cuff.
It is important to maintain the strength in the muscles of the rotator cuff. These muscles help control the stability of the shoulder joint. Strengthening these muscles can actually decrease the impingement of the acromion on the rotator cuff tendons and bursa. Your therapist can also evaluate your workstation or the way you use your body when you do your activities and suggest changes to avoid further problems.
Rehabilitation after shoulder surgery can be a slow process. You will probably need to attend therapy sessions for several weeks, and you should expect full recovery to take several months. Getting the shoulder moving as soon as possible is important. However, this must be balanced with the need to protect the healing muscles and tissues.
Your surgeon may have you wear a sling to support and protect the shoulder for a few days after surgery. Ice and electrical stimulation treatments may be used during your first few therapy sessions to help control pain and swelling from the surgery. Your therapist may also use massage and other types of hands-on treatments to ease muscle spasm and pain.
Therapy can progress quickly after a simple arthroscopic procedure. Treatments start out with range-of-motion exercises and gradually work into active stretching and strengthening. You just need to be careful to avoid doing too much, too quickly.
Therapy goes slower after open surgery in which the shoulder muscles have been cut. Therapists will usually wait up to two weeks before starting range-of-motion exercises. Exercises begin with passive movements. During passive exercises, your shoulder joint is moved, but your muscles stay relaxed. Your therapist gently moves your joint and gradually stretches your arm. You may be taught how to do passive exercises at home.
Active therapy starts four to six weeks after surgery. You use your own muscle power in active range-of-motion exercises. You may begin with light isometric strengthening exercises. These exercises work the muscles without straining the healing tissues.
At about six weeks you start doing more active strengthening. Exercises focus on improving the strength and control of the rotator cuff muscles and the muscles around the shoulder blade. Your therapist will help you retrain these muscles to keep the ball of the humerus in the socket. This helps your shoulder move smoothly during all your activities.
Some of the exercises you’ll do are designed get your shoulder working in ways that are similar to your work tasks and sport activities. Your therapist will help you find ways to do your tasks that don’t put too much stress on your shoulder. Before your therapy sessions end, your therapist will teach you a number of ways to avoid future problems.
https://www.youtube.com/watch?v=cyXf5YbnJKs Artificial Hip Replacement Anterior Approach (Hip Arthroplasty)
https://www.youtube.com/watch?v=m8LDBlZN-XM Artificial Knee Replacement (Knee Arthroplasty) Animated Tutorial
https://www.youtube.com/watch?v=0qR-Yfw9fOI Lumbar Spine Anatomy Animated Tutorial
https://www.youtube.com/watch?v=RNUpMNd_u1U Cervical Spine Anatomy Animated Tutorial
https://www.youtube.com/watch?v=qlCvKEOZtpo Hip Anatomy Animated Tutorial
https://www.youtube.com/watch?v=_q-Jxj5sT0g Knee Anatomy Animated Tutorial
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}