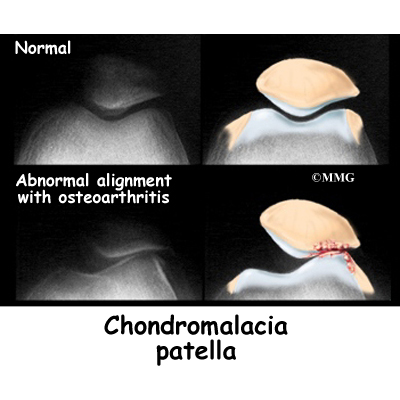
The patella, or kneecap, can be a source of knee pain when it fails to function properly. Alignment or overuse problems of the patella can lead to wear and tear of the cartilage behind the patella. Chondromalacia patella is a common knee problem that affects the patella and the groove it slides in over the femur (thigh bone). This action takes place at the patellofemoral joint.
Chondromalacia is the term used to describe a patellofemoral joint that has been structurally damaged, while the term patellofemoral pain syndrome (PFPS) refers to the earlier stages of the condition. Symptoms are more likely to be reversible with PFPS.
This guide will help you understand
What is the patella, and what does it do?
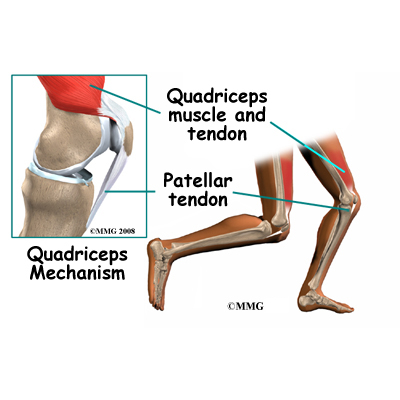
The patella (kneecap) is the moveable bone on the front of the knee. This unique bone is wrapped inside a tendon that connects the large muscles on the front of the thigh, the quadriceps muscles, to the lower leg bone. The large quadriceps tendon together with the patella is called the quadriceps mechanism. Though we think of it as a single device, the quadriceps mechanism has two separate tendons, the quadriceps tendon on top of the patella and the patellar tendon below the patella.
Tightening up the quadriceps muscles places a pull on the tendons of the quadriceps mechanism. This action causes the knee to straighten. The patella acts like a fulcrum to increase the force of the quadriceps muscles.
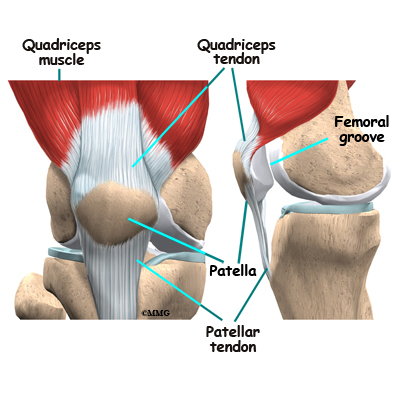
The underside of the patella is covered with articular cartilage, the smooth, slippery covering found on joint surfaces. This covering helps the patella glide (or track) in a special groove made by the thighbone, or femur. This groove is called the femoral groove.
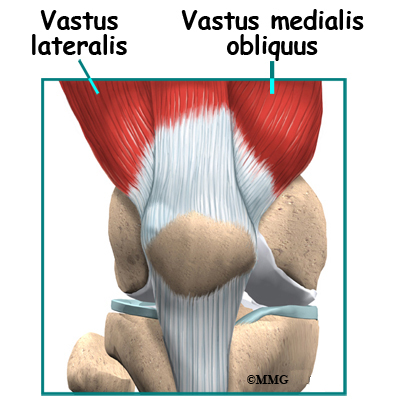
Two muscles of the thigh attach to the patella and help control its position in the femoral groove as the leg straightens. These muscles are the vastus medialis obliquus (VMO) and the vastus lateralis (VL). The vastus medialis obliquus (VMO) runs along the inside of the thigh, and the vastus lateralis (VL) lies along the outside of the thigh. If the timing between these two muscles is off, the patella may be pulled off track.
Related Document: A Patient’s Guide to Knee Anatomy
What causes this problem?
Problems commonly develop when the patella suffers wear and tear. The underlying cartilage begins to degenerate, a condition most common in young athletes. Soccer players, snowboarders, cyclists, rowers, tennis players, ballet dancers, and runners are affected most often. But anyone whose knees are under great stress is at increased risk of developing chondromalacia patella.
Wear and tear can develop for several reasons. Acute injury to the patella or chronic friction between the patella and the femur can result in the start of patellofemoral pain syndrome. Degeneration leading to chondromalacia may also develop as part of the aging process, like putting a lot of miles on a car.
The main cause of knee pain associated with patellofemoral pain syndrome is a problem in the way the patella tracks within the femoral groove as the knee moves. Physical and biomechanical changes alter the stress and load on the patellofemoral joint.
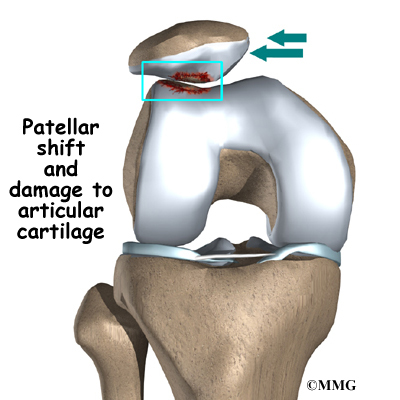
The quadriceps muscle helps control the patella so it stays within this groove. If part of the quadriceps is weak for any reason, a muscle imbalance can occur. When this happens, the pull of the quadriceps muscle may cause the patella to pull more to one side than the other. This in turn causes more pressure on the articular cartilage on one side than the other. In time, this pressure can damage the articular cartilage leading to chondromalacia patella.
Weakness of the muscles around the hip can also indirectly affect the patella and can lead to patellofemoral joint pain. Weakness of the muscles that pull the hip out and away from the other leg, the hip abductor muscles, can lead to imbalances to the alignment of the entire leg – including the knee joint and the muscle balance of the muscles around the knee. This causes abnormal tracking of the patella within the femoral groove and eventually pain around the patella. Many patients are confused when their physical therapist begins exercises to strengthen and balance the hip muscles, but there is a very good reason that the therapist is focusing on this area.
A similar problem can happen when the timing of the quadriceps muscles is off. There are four muscles that form the quadriceps muscle group. As mentioned earlier, the vastus medialis obliquus (the muscle on the inside of the front of the thigh) and the vastus lateralis ( the muscle that runs down the outside part of the thigh) are two of these four muscles. People with patellofemoral problems sometimes have problems in the timing between the VMO and the VL. The VL contracts first, before the VMO. This tends to pull the patella toward the outside edge of the knee. The result is abnormal pressure on the articular surface of the patella.
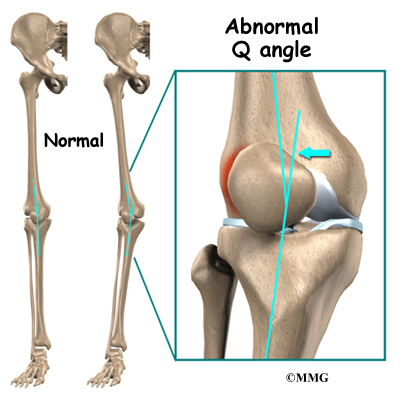
Another type of imbalance may exist due to differences in how the bones of the knee are shaped. These differences, or anatomic variations, are something people are born with. Doctors refer to this the “Q angle”. Some people are born with a greater than normal angle where the femur and the tibia (shinbone) come together at the knee joint. Women tend to have a greater angle here than men. The patella normally sits at the center of this angle within the femoral groove. When the quadriceps muscle contracts, the angle in the knee straightens, pushing the patella to the outside of the knee. In cases where this angle is increased, the patella tends to shift outward with greater pressure. This leads to a similar problem as that described above. As the patella slides through the groove, it shifts to the outside. This places more pressure on one side than the other, leading to damage to the underlying articular cartilage.
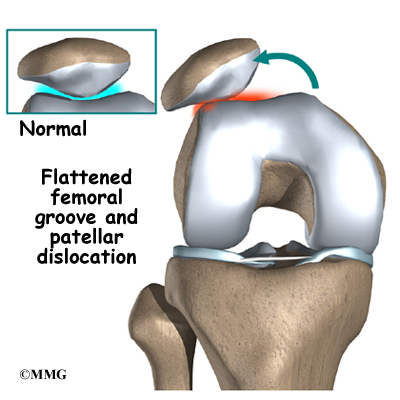
Finally, anatomic variations in the bones of the knee can occur such that one side of the femoral groove is smaller than normal. This creates a situation where the groove is too shallow, usually on the outside part of the knee. People who have a shallow groove sometimes have their patella slip sideways out of the groove, causing a patellar dislocation. This is not only painful when it occurs, but it can damage the articular cartilage underneath the patella. If this occurs repeatedly, degeneration of the patellofemoral joint occurs fairly rapidly.
What does chondromalacia patella feel like?
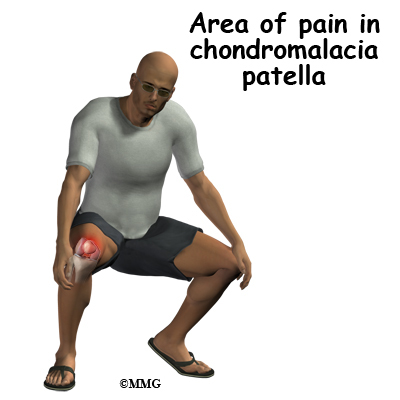
The most common symptom is pain underneath or around the edges of the patella. The pain is made worse by any activities that load the patellofemoral joint, such as running, squatting, or going up and down stairs. Kneeling is often too painful to even try. Keeping the knee bent for long periods, as in sitting in a car or movie theater, may cause pain.
There may be a sensation like the patella is slipping. This is thought to be a reflex response to pain and not because there is any instability in the knee. Others experience vague pain in the knee that isn’t centered in any one spot.
The knee may grind, or you may hear a crunching sound when you squat or go up and down stairs. If there is a considerable amount of wear and tear, you may feel popping or clicking as you bend your knee. This can happen when the uneven surface of the underside of the patella rubs against the femoral groove. The knee may swell with heavy use and become stiff and tight. This is usually because of fluid accumulating inside the knee joint, sometimes called ‘water on the knee’. This is not unique to problems of the patella but sometimes occurs when the knee becomes inflamed.
How do doctors diagnose the problem?
Diagnosis begins with a complete history of your knee problem followed by an examination of the knee, including the patella. X-rays may be ordered on the initial visit to your doctor. An X-ray can help determine if the patella is properly aligned in the femoral groove. Several X-rays taken with the knee bent at several different angles can help determine if the patella seems to be moving through the femoral groove in the correct alignment. The X-ray may show arthritis between the patella and thighbone, especially when the problems have been there for awhile.
Diagnosing problems with the patella can be confusing. The symptoms can be easily confused with other knee problems, because the symptoms are often similar. In these cases, other tests, such as magnetic resonance imaging (MRI), may be suggested. The MRI machine uses magnetic waves rather than X-rays to show the soft tissues of the body. This machine creates pictures that look like slices of the knee. Usually, this test is done to look for injuries, such as tears in the menisci or ligaments of the knee. Recent advances in the quality of MRI scans have enabled doctors to see the articular cartilage on the scan and determine if it is damaged. This test does not require any needles or special dye and is painless.
In some cases, arthroscopy may be used to make the definitive diagnosis when there is still a question about what is causing your knee problem. Arthroscopy is an operation that involves placing a small fiber-optic TV camera into the knee joint, allowing the surgeon to look at the structures inside the joint directly. The arthroscope allows your doctor to see the condition of the articular cartilage on the back of your patella. The vast majority of patellofemoral problems are diagnosed without resorting to surgery, and arthroscopy is usually reserved to treat the problems identified by other means.
There is no clear link between the severity of symptoms and X-ray or arthroscopic findings. Most often, the doctor relies upon the history, symptoms, and results of the examination.
What treatment options are available?
Nonoperative treatment is usually recommended for this problem. Getting the pain and inflammation under control is the first step. The overall goals for a rehab plan are to improve muscle function and flexibility while providing pain relief or pain control.
Your physician may suggest rest and anti-inflammatory medications, such as aspirin or ibuprofen, especially when the problem is coming from overuse. Acetaminophen (Tylenol®) may be used for pain control if you can’t take anti-inflammatory medications for any reason. Activity modification, flexibility, and strengthening are key parts of the rehab program. Physical therapy can help in the early stages by decreasing pain and inflammation. Your physical therapist may use ice massage and ultrasound to limit pain and swelling.
Bracing or taping the patella can help you do exercises and activities with less pain. Most braces for patellofemoral problems are made of soft fabric, such as cloth or neoprene. You slide them onto your knee like a sleeve. A small buttress pads the side of the patella to keep it lined up within the groove of the femur.
An alternative to bracing is to tape the patella in place. The therapist applies and adjusts the tape over the knee to help realign the patella. The idea is that by bracing or taping the knee, the patella stays in better alignment within the femoral groove. This in turn is thought to improve the pull of the quadriceps muscle so that the patella stays lined up in the groove. Patients report less pain and improved function with these forms of treatment.
As the pain and inflammation become controlled, your physical therapist will work with you to improve flexibility, strength, and muscle balance in the knee. Quadriceps strengthening exercises to address deficits in knee extension strength include non-weight-bearing single-joint (e.g., knee extension) and weight-bearing multiple-joint exercises (e.g., seated leg press).
Non-weight bearing exercises are also known as open kinetic chain exercise. Weight-bearing exercises are referred as closed-chain exercise. Closed-chain exercises place less stress on the patellofemoral joint and may be used first to achieve improved function before progressing to open kinetic chain exercises. Studies also show greater VMO activity with closed kinetic chain exercise. And a closed-chain exercise program also addresses hip muscle weakness at the same time as knee muscle deficits.
The therapist will adjust your rehab program to provide you with the most pain free and effective method of treatment. The overall rehab program will include a home exercise program of stretching, agility exercises, balance activities, and strengthening designed to return you to your former level of pain free participation in sports and other activities.
If nonsurgical treatment fails to improve your condition, surgery may be suggested. The procedure used for patellofemoral problems varies. In severe cases a combination of one or more of the following procedures may be necessary.
Arthroscopic Method
Arthroscopy is sometimes useful in the treatment of patellofemoral problems of the knee. Looking directly at the articular cartilage surfaces of the patella and the femoral groove is the most accurate way of determining how much wear and tear there is in these areas. Your surgeon can also watch as the patella moves through the groove, and may be able to decide whether or not the patella is moving normally. If there are areas of articular cartilage damage behind the patella that are creating a rough surface, special tools can be used by the surgeon to smooth the surface and reduce your pain. This procedure is sometimes referred to as shaving the patella.
Cartilage Procedure
In more advanced cases of patellar arthritis, surgeons may operate to repair or restore the damaged cartilage. The type of surgery needed for articular cartilage is based on the size, type, and location of the damage. Along with surgical treatment to fix the cartilage, other procedures may also be done to help align the patella so less pressure is placed on the healing cartilage.
Related Document: A Patient’s Guide to Articular Cartilage Problems of the Knee
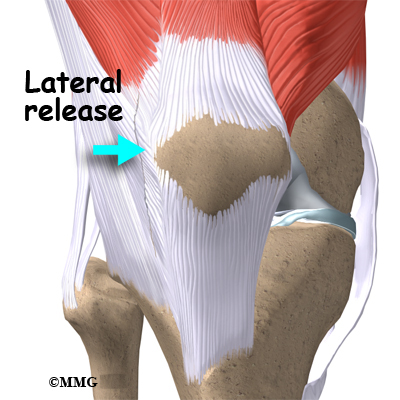
Lateral Release
If your patella problems appear to be caused by a misalignment problem, a procedure called a lateral release may be suggested. This procedure is done to allow the patella to shift back to a more normal position and relieve pressure on the articular cartilage.
In this operation, the tight ligaments on the outside (lateral side) of the patella are cut, or released, to allow the patella to slide more towards the center of the femoral groove. These ligaments eventually heal with scar tissue that fills in the gap created by the surgery, but they no longer pull the patella to the outside as strongly as before the surgery. This helps to balance the quadriceps mechanism and equalize the pressure on the articular cartilage behind the patella.
Ligament Tightening Procedure
In some cases of severe patellar misalignment, a lateral release alone may not be enough. For problems of repeated patellar dislocations, the surgeon may also need to realign the quadriceps mechanism. In addition to the lateral release, the tendons on the inside edge of the knee (the medial side) may have to be tightened as well.
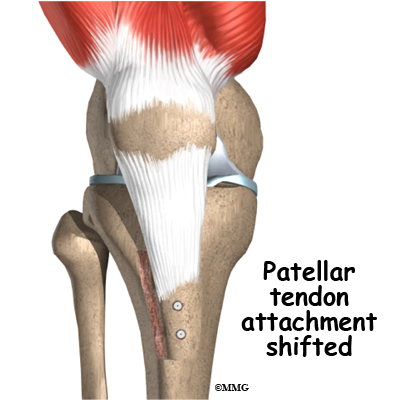
Bony Realignment
If the misalignment is severe, the bony attachment of the patellar tendon may also have to be shifted to a new spot on the tibia bone. Remember that the patellar tendon attaches the patella to the lower leg bone (tibia) just below the knee. By moving a section of bone where the patellar tendon attaches to the tibia, surgeons can change the way the tendon pulls the patella through the femoral groove.
The surgeon removes a section of bone where the patellar tendon attaches on the tibia. This section of bone is then reattached on the tibia closer to the other knee.
Usually, the bone is reattached onto the tibia using screws. This procedure shifts the patella to the medial side. Once the surgery heals, the patella should track better within the center of the groove, spreading the pressure equally on the articular cartilage behind the patella.
Arthroscopic procedures to shave the patella or a simple lateral release can usually be done on an outpatient basis, meaning you can leave the hospital the same day. If your problem requires the more involved surgical procedure where bone must be cut to allow moving the patellar tendon attachment, you may need to spend one or two nights in the hospital.
What should I expect after treatment?
Patients with chondromalacia may benefit from four to six weeks of physical therapy. The aim of treatment is to calm pain and inflammation, to correct muscle imbalances, and to improve function of the patella.
It is important to understand the need to keep your activity level below what will trigger more pain and tissue damage. You may need to ice your knee during the day and limit certain activities such as stairs, squatting, or running.
Good results can be expected when working slowly but steadily on flexibility and strengthening exercises. The moto of no pain, no gain does not apply to this problem. The most successful program is one of common sense. If an activity causes pain, then reduce the frequency, intensity, or duration of that activity until you are once again pain free. Gradually build up what you can do while maintaining your pain free status.
Muscle imbalances are commonly treated with stretching and strengthening exercises but improvement usually takes at least six to eight weeks. You may need to continue a modified program of flexibility and strengthening exercises to maximize control and strength of the quadriceps muscles. This type of program done two to three times each week may be needed for several more months (or longer if you continue to experience pain during progressive sports participation).
Many surgeons will have their patients take part in formal physical therapy after knee surgery for patellofemoral problems. Patients undergoing a patellar shaving usually begin rehabilitation right away. More involved surgeries for patellar realignment or restorative procedures for the articular cartilage require a delay before going to therapy. And rehabilitation may be slower to allow the bone or cartilage to heal before too much strain can be put on the knee.
The first few physical therapy treatments are designed to help control the pain and swelling from the surgery. The physical therapist will choose exercises to help improve knee motion and to get the quadriceps muscles toned and active again. Muscle stimulation, using electrodes over the quadriceps muscle, may be needed at first to get the muscle moving again.
As the program evolves, more challenging exercises are chosen to safely advance the knee’s strength and function. The key is to get the soft tissues in balance through safe stretching and gradual strengthening.
The physical therapist’s goal is to help you keep your pain under control, ensure you place only a safe amount of weight on the healing knee, and improve your strength and range of motion. When you are well under way, regular visits to the therapist’s office will end. The therapist will continue to be a resource, but you will be in charge of doing your exercises as part of an ongoing home program.
https://www.youtube.com/watch?v=cyXf5YbnJKs Artificial Hip Replacement Anterior Approach (Hip Arthroplasty)
https://www.youtube.com/watch?v=m8LDBlZN-XM Artificial Knee Replacement (Knee Arthroplasty) Animated Tutorial
https://www.youtube.com/watch?v=0qR-Yfw9fOI Lumbar Spine Anatomy Animated Tutorial
https://www.youtube.com/watch?v=RNUpMNd_u1U Cervical Spine Anatomy Animated Tutorial
https://www.youtube.com/watch?v=qlCvKEOZtpo Hip Anatomy Animated Tutorial
https://www.youtube.com/watch?v=_q-Jxj5sT0g Knee Anatomy Animated Tutorial
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}