Lumbar Spine
Lumbar Spine Anatomy
A Patient’s Guide to Lumbar Spine Anatomy
Introduction
Knowing the main parts of your low back and how these parts work is important as you learn to care for your back problem.
Two common anatomic terms are useful as they relate to the low back. The term anterior refers to the front of the spine. The term posterior refers to the back of the spine. The section of the spine that makes up the low back is called the lumbar spine. The front of the low back is therefore called the anterior lumbar area. The back of the lower spine is called the posterior lumbar area.
In addition to reading this article, be sure to watch our Lumbar Spine Anatomy Animated Tutorial Video.
This guide gives a general overview of the anatomy of the low back. It should help you understand
- what parts make up the low back
- how these parts work
Important Structures
The important parts of the lumbar spine include
- bones and joints
- nerves
- connective tissues
- muscles
- spinal segments
This section highlights important structures in each category.
Bones and Joints
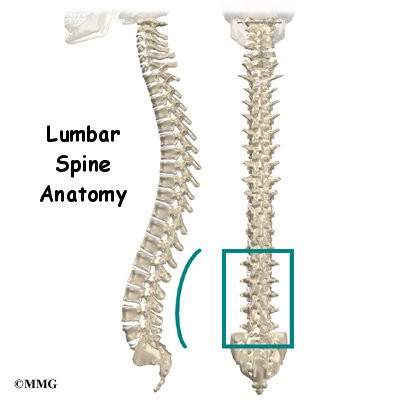
The human spine is made up of 24 spinal bones, called vertebrae. Vertebrae are stacked on top of one another to form the spinal column. The spinal column is the body’s main upright support.
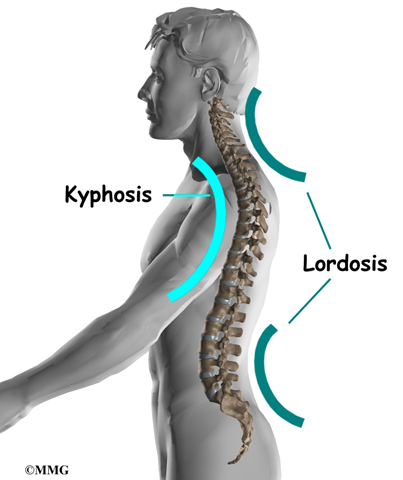
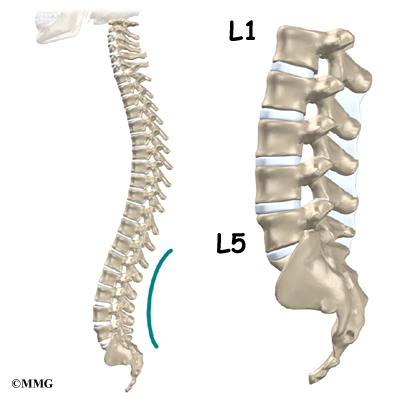
From the side, the spine forms three curves. The neck, called the cervical spine curves slightly inward.
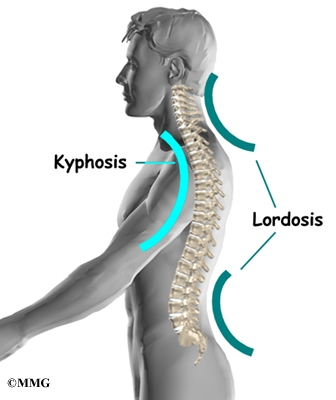
The middle back, or thoracic spine curves outward. The outward curve of the thoracic spine is called kyphosis. The low back, also called the lumbar spine curves slightly inward. An inward curve of the spine is called lordosis.

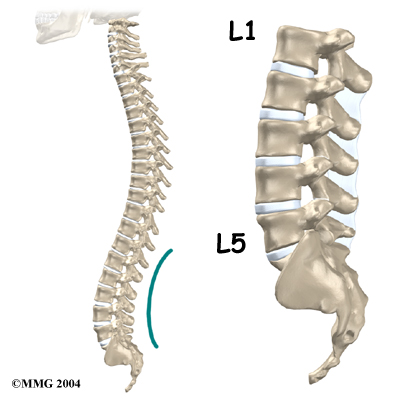
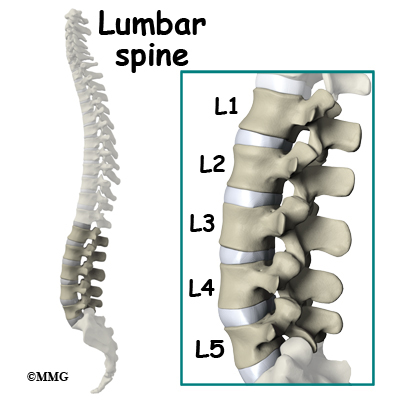
The lumbar spine is made up of the lower five vertebrae. Doctors often refer to these vertebrae as L1 to L5. The lowest vertebra of the lumbar spine, L5, connects to the top of the sacrum, a triangular bone at the base of the spine that fits between the two pelvic bones. Some people have an extra, or sixth, lumbar vertebra. This condition doesn’t usually cause any particular problems.
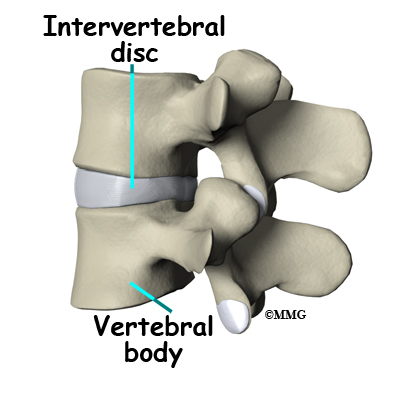
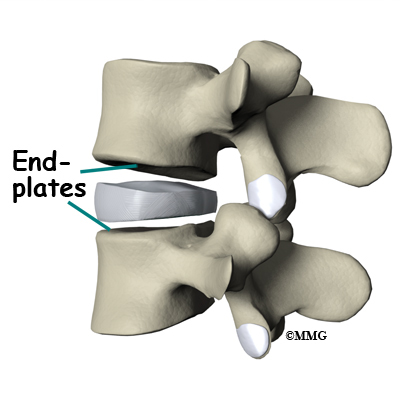
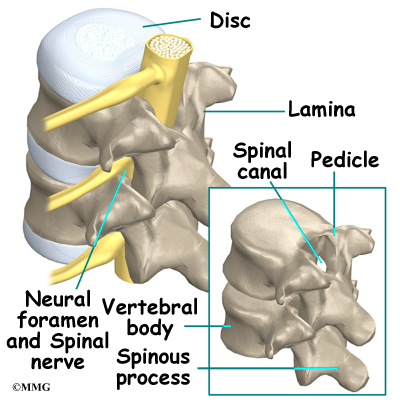
Each vertebra is formed by a round block of bone, called a vertebral body. The lumbar vertebral bodies are taller and bulkier compared to the rest of the spine. This is partly because the low back has to withstand pressure from body weight and from movements such as lifting, carrying, and twisting. Also, large and powerful muscles attaching on or near the lumbar spine place extra force on the lumbar vertebral bodies.
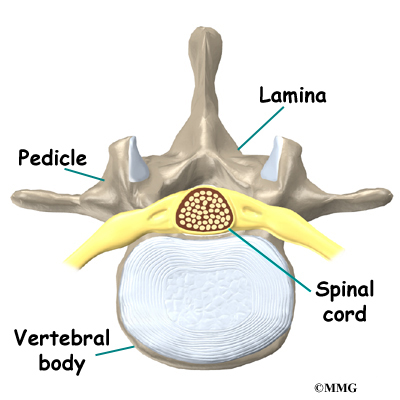
A bony ring attaches to the back of each vertebral body. This ring has two parts. Two pedicle bones connect directly to the back of the vertebral body. Two lamina bones join the pedicles to complete the ring. The lamina bones form the outer rim of the bony ring. When the vertebrae are stacked on top of each other, the bony rings form a hollow tube that surrounds the spinal cord and nerves. The laminae provide a protective roof over these nerve tissues.

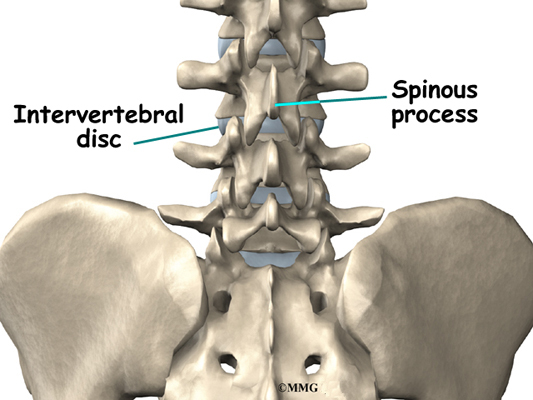
A bony knob projects out at the point where the two lamina bones join together at the back of the spine. These projections, called spinous processes, can be felt as you rub your fingers up and down the back of your spine. Each vertebra also has two bony knobs that point out to the side, one on the left and one on the right. These bony projections are called transverse processes. The projections in the low back are broader than in other areas of the spine because many large back muscles attach and impart powerful forces on them.
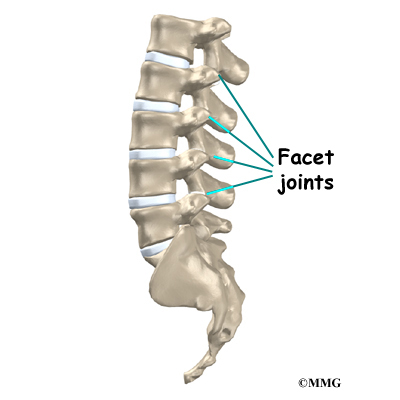
Between the vertebrae of each spinal segment are two facet joints. The facet joints are located on the back of the spinal column. There are two facet joints between each pair of vertebrae, one on each side of the spine. A facet joint is made of small, bony knobs that line up along the back of the spine. Where these knobs meet, they form a joint that connects the two vertebrae. The alignment of the facet joints of the lumbar spine allows freedom of movement as you bend forward and back.
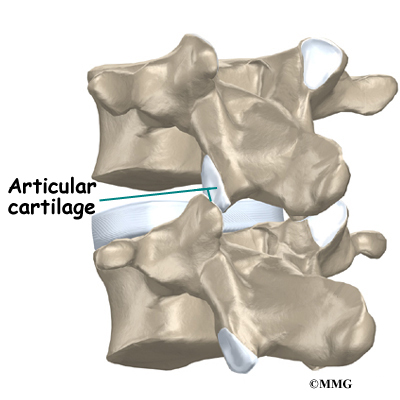
The surfaces of the facet joints are covered by articular cartilage. Articular cartilage is a smooth, rubbery material that covers the ends of most joints. It allows the ends of bones to move against each other smoothly, without friction.
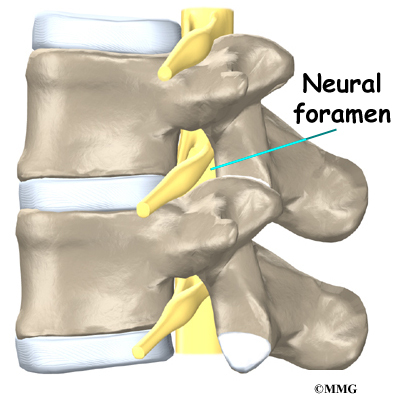
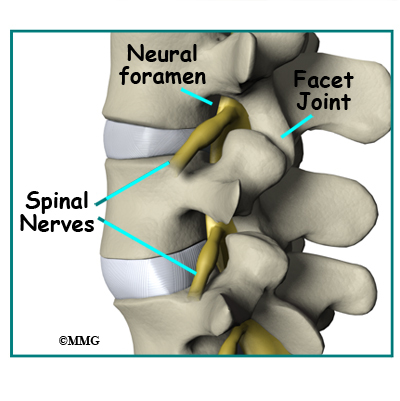
On the left and right side of each vertebra is a small tunnel called a neural foramen. (Foramina is the plural term.) The two nerves that leave the spine at each vertebra go through the foramina, one on the left and one on the right. The intervertebral disc (described later) sits directly in front of the opening. A bulged or herniated disc can narrow the opening and put pressure on the nerve. A facet joint sits in back of the foramen. Bone spurs that form on the facet joint can project into the tunnel, narrowing the hole and pinching the nerve.
Nerves
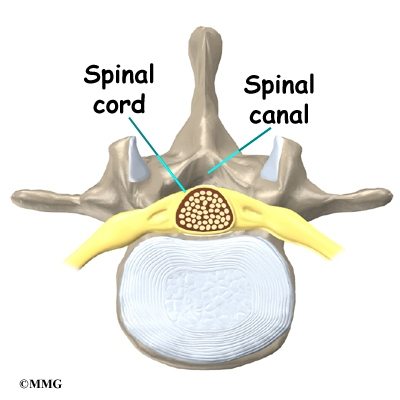
The hollow tube formed by the bony rings on the back of the spinal column surrounds the spinal cord. The spinal cord is like a long wire made up of millions of nerve fibers. Just as the skull protects the brain, the bones of the spinal column protect the spinal cord.
The spinal cord extends down to the L2 vertebra. Below this level, the spinal canal encloses a bundle of nerves that goes to the lower limbs and pelvic organs. The Latin term for this bundle of nerves is cauda equina meaning horse’s tail.
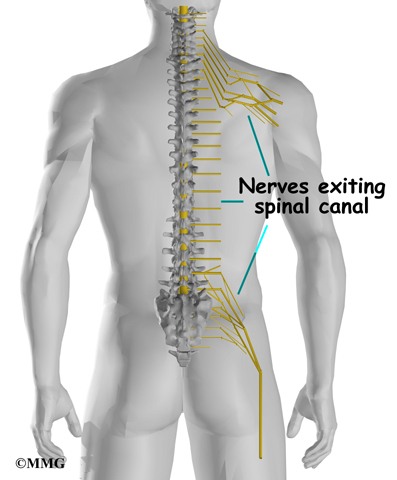
Between vertebrae, two large nerves branch off the spinal cord, one on the left and one on the right. The nerves pass through the neural foramina of each vertebra. These spinal nerves group together to form the main nerves that go to the organs and limbs. The nerves of the lumbar spine (cauda equina) go to the pelvic organs and lower limbs.
Connective Tissues

Connective tissues are networks of fiber that hold the cells of the body together. Ligaments are strong connective tissues that attach bones to other bones. Several long ligaments connect on the front and back sections of the vertebrae. The anterior longitudinal ligament runs lengthwise down the front of the vertebral bodies. Two other ligaments run full-length within the spinal canal. The posterior longitudinal ligament attaches on the back of the vertebral bodies. The ligamentum flavum is a long elastic band that connects to the front surface of the lamina bones (just behind the spinal cord). Thick ligaments also connect the bones of the lumbar spine to the sacrum (the bone below L5) and pelvis.
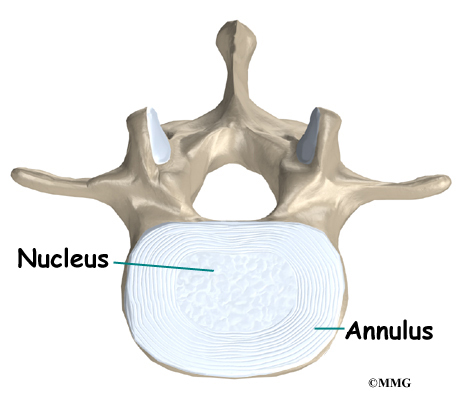
A special type of structure in the spine called an intervertebral disc is also made of connective tissue. The fibers of the disc are formed by special cells, called collagen cells. The fibers may be lined up like strands of nylon rope or crisscrossed like a net.
An intervertebral disc is made of two parts. The center, called the nucleus, is spongy. It provides most of the shock absorption in the spine. The nucleus is held in place by the annulus, a series of strong ligament rings surrounding it.
Muscles
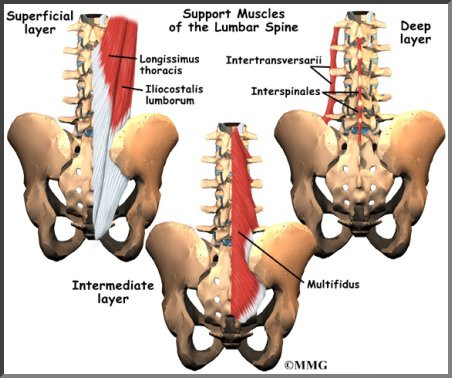
The muscles of the low back are arranged in layers. Those closest to the skin’s surface, the superficial layer, are covered by a thick tissue called fascia. The middle layer, called the erector spinae, has strap-shaped muscles that run up and down over the lower ribs, chest, and low back. They join in the lumbar spine to form a thick tendon that binds the bones of the low back, pelvis, and sacrum. The deepest layer of muscles attaches along the back surface of the spine bones, connecting the low back, pelvis, and sacrum. These deepest muscles coordinate their actions with the muscles of the abdomen to help hold the spine steady during activity.
Spinal Segment
A good way to understand the anatomy of the lumbar spine is by looking at a spinal segment. Each spinal segment includes two vertebrae separated by an intervertebral disc, the nerves that leave the spinal column at each vertebra, and the small facet joints that link each level of the spinal column.
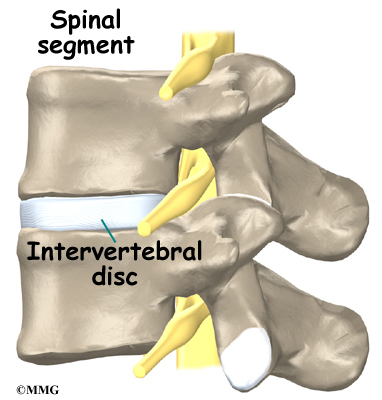
The intervertebral disc separates the two vertebral bodies of the spinal segment. The disc normally works like a shock absorber. It protects the spine against the daily pull of gravity. It also protects the spine during heavy activities that put strong force on the spine, such as jumping, running, and lifting.
The spinal segment is connected by two facet joints, described earlier. When the facet joints of the lumbar spine move together, they bend and turn the low back.
Summary
Many important parts make up the anatomy of the back. Understanding the regions and structures of the lumbar spine can help you be more involved in your health care and better able to care for your back problem.
Transcutaneous Electrical Stimulation (TENS) for Chronic Lumbar Spine Pain
A Patient’s Guide to Transcutaneous Electrical Stimulation (TENS) for Chronic Lumbar Spine Pain
Introduction
Low back pain due to musculoskeletal disorders, is the largest cause of time off work. The most commonly prescribed intervention is rest, pain medications, and a referral to physical therapy.
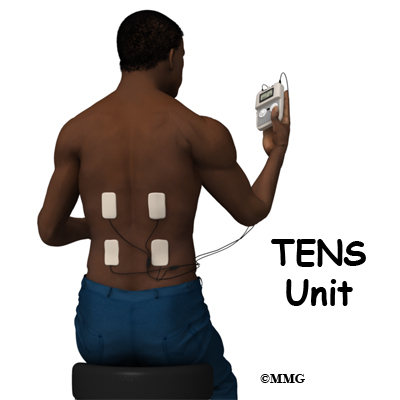
Physicians and physical therapists commonly recommend the use of a transcutaneous electrical nerve stimulation (TENS) unit as part of a pain management strategy for controlling low back pain. TENS is used primarily for chronic pain.
This guide will help you understand
- who may benefit from a TENS unit
- how a TENS unit works
- what to expect with a TENS unit
Who may benefit from a TENS?
TENS can be used for relief of pain associated with a wide variety of painful conditions. This may include back pain caused by spine degeneration, disc problems, or failed back surgery. Nerve pain from conditions such as chronic regional pain syndrome (CRPS) and neuropathies caused by diabetes or as a side effect of cancer treatment may also be managed with TENS.
TENS has been used for people suffering from cancer-related pain, phantom-limb pain (a chronic pain syndrome following limb amputation), and migraine or chronic tension-type headaches.
TENS can also be used for muscle soreness from overuse, inflammatory conditions, and both rheumatoid and osteoarthritis. Athletes with painful acute soft tissue injuries (e.g., sprains and strains) may benefit from TENS treatment.
Sometimes it is used after surgery for incisional or post-operative pain from any type of surgery (e.g., joint replacement, cardiac procedures, various abdominal surgeries, cesaerean section for the delivery of a baby). Studies show that TENS can significantly reduce the use of analgesics (pain relievers, including narcotic drugs) after surgery.
TENS is usually used along with other forms of treatment and pain control such as analgesics, relaxation therapy, biofeedback, visualization or guided imagery, physical therapy and exercise, massage therapy, nerve block injections, and/or spinal manipulation.
The effectiveness of TENS remains controversial. The American Academy of Neurology (AAN) findings published in Dec. 30, 2009 issue of Neurology claims it is not effective and cannot be recommended. But, many patients find TENS effective for pain relief, easy to use, and with very low side effects. It may be worth a try for those who suffer from chronic low back pain. It can be discontinued easily if it doesn’t work. TENS cannot correct an underlying problem; it is only used for temporary relief of symptoms.
TENS is a noninvasive way to override or block signals from the nerves to the spinal cord and brain. Pain messages may be altered enough to provide temporary pain relief. Besides controlling pain, this type of electrical stimulation can also improve local circulation and reduce or eliminate muscle spasm.
To summarize, the benefits from TENS treatment can include:
- pain relief
- increased circulation and healing
- improved sleep pattern
- decreased use of pain relievers or other analgesic drugs
- increased motion and function
How does a TENS work?
TENS produces an electrical impulse that can be adjusted for pulse, frequency, and intensity. The exact mechanism by which it works to reduce or even eliminate pain is still unknown. It is possible there are several different ways TENS works. For example, TENS may inhibit (block) pain pathways or increase of the secretion of the pain reducing substances (e.g., endorphins, serotonin) in the CNS.
Electrical stimulation has been shown to enhance tissue healing by improving circulation. This effect may alter pain perception.
Some integrative medicine practitioners also believe that it’s possible that the flow of energy through the meridian system modifies the sensation of pain. These practitioners believe that meridians are interconnected channels of energy throughout the body that are closely linked with the central nervous system (brain and spinal cord) as well as the peripheral nervous system (spinal nerves). These practitioners suggest that the electrical stimulation from the TENS unit is able to open up any blocked areas of energy flow bringing pain relief.
Recent research has also shown that autosuggestion or the placebo effect is a powerful way many people experience pain relief or improvement in symptoms. Simply by believing the treatment (any treatment, including TENS) will work has a beneficial effect on the nervous system. Many studies have shown that people get pain relief through the placebo effect alone.
How do I use my TENS unit
You will be shown how to use your TENS device by your healthcare provider trained in the set-up and use of this modality. Round or square rubber electrodes are applied to the skin over or around the painful area. Usually four electrodes (two pairs) are used to get maximum benefit from this treatment.
The electrodes are self-adhesive with a protective layer of gel built in to prevent skin irritation or burning. The unit is battery-operated with controls you manipulate yourself to alter the strength of the electrical signal. The unit can be slipped into a pocket or clipped to your belt. You may use two or four electrodes.
The electrodes will be placed on your body at positions selected by a physician or physical therapist. The electrode placement is determined based on the location of the involved nerves and/or the location of your pain.
The first place to try the electrodes is either directly over the painful area or on either side of the pain. You will slowly turn up the intensity of the unit until you feel a buzzing, tingling, or thumping sensation strong enough to override the pain signals.
If that doesn’t work, you may get better results putting the electrodes over the area where the spinal nerve root exits the vertebra. Sometimes it takes a bit of trial and error to find the right settings and best electrode placement for you.
Be sure and let your healthcare provider know if you experience increased pain. Electrodes placed below the level of a peripheral nerve impairment might actually block the input from the TENS unit and cause increased pain. Or placement over an area of scar tissue from surgery can cause increased skin resistance and decreased transmission of the electrical impulses.
Another way to use TENS is over spots in the muscles that trigger pain called trigger points (TrPs). Trigger points are areas of hyperirritability in the muscles that can cause chronic pain. The healthcare provider will identify any TrPs present during your exam. Usually TrPs are taken care of with a treatment designed to eliminate them. In some patients they are chronic and don’t go away or come back easily. In such cases, TENS may be helpful.
Your health care team will guide you through the trial-and-error process for finding the best electrode placement for you and make any changes needed in the program.
When you should NOT use TENS
1.If you have loss of skin sensation or even decreased sensation, you should not use TENS. With altered sensation, there is a risk of turning the unit up too high and causing injury or harm.
2.The use of TENS is not recommended for older adults with Alzheimer’s, dementia, or other cognitive problems.
3.If you have a cardiac pacemaker, you should not use TENS as the electrical signals could interfere with your pacemaker. Cardiac patients should not use TENS without their physician’s approval.
Some guidelines when using TENS
- Before applying the electrodes, it is important to remove all lotions, oils, or other applications to the skin. You may want to shave hair from the local area where the electrode will be applied.
- Daily use of TENS for several hours at a time is recommended. You should not wear the unit for long periods of time (e.g., 24 hours) or during extended sleep time (napping is okay but TENS should not be used while sleeping at night or for more than a couple of hours).
- Never place an electrode over an open wound or area of skin irritation. Report any skin problems or burns immediately.
- Do not place electrodes near your eyes or over your throat.
- Do not use TENS in the shower or bathtub.
- Move the electrodes a bit each time you put them on to avoid skin irritation.
- You should experience a comfortable tingling sensation that is comfortable enough to allow you to complete daily tasks and activities.
- You may want to keep a daily journal of your pain levels, the settings you use, and a record of the medications you are taking for pain relief. By reviewing your notes, you may find the best combination of electrode placement and unit settings that gives you the most pain relief.
What can you expect with TENS
You should feel a mild to moderately strong tingling or buzzing sensation. Some people experience a more unpleasant sensation described as burning or prickling. Depending on the intensity and duration of your pain, you may or may not get results right away.
It can take several days to even several weeks to get the desired results. Differences in results may occur based on properties of skin resistance, type of pain, and individual differences in the mechanism of pain control. Be patient and persistent. Do not hesitate to contact your healthcare provider as often as it takes to get the desired results.
Many patients do report good-to-excellent results, first with pain control, then pain relief, and finally reduction in the use of medications. Although it doesn’t happen for everyone, some chronic pain patients are “cured” permanently from their pain.
As each of these benefits from the TENS treatment occur, you may find yourself increasing your activity level – either with the same level of TENS usage or even with reduced frequency of use, intensity of signal, or duration (length of time the unit is turned on).
If for any reason your pain starts to increase in frequency, duration, or intensity, don’t assume the treatment isn’t working for you. First, check the TENS unit for any malfunction, need to recharge, or replace the electrodes with new ones. If your unit is battery-operated, you may find it necessary to turn the intensity up to obtain the same sensation when the batteries are low. This should alert you to the need for battery replacement.
Finally, be aware that some patients experience “breakthrough pain,” referring to a situation in which you get pain relief at first but then even with the TENS unit, you start to have pain once again. Turning the intensity up high enough to cause muscle contraction is an indication of breakthrough pain.
Sometimes a different setting for the stimulator may be needed when this happens. Most units have a setting that allows for random pulse frequency, duration, and amplitude. The use of this setting helps keep the nervous system from getting used to a specific amount of stimulation and ignoring it. This phenomenon is called habituation or adaptation.
Summary
TENS is an effective method of pain control for chronic pain when you want to maintain your normal routine of daily activities that would otherwise be hampered by too high of pain levels. TENS helps many people reduce and sometimes even eliminate the use of pain medications, thus avoiding side-effects of long-term drug use.
Even without complete pain relief, TENS makes it possible to stay active and participate in work, family, and even recreational activities. There are no significant adverse effects from the use of TENS. The ability of this treatment technique to moderate pain and reduce the use of pain medications is a real benefit — especially with the potential for serious or adverse effects from long-term use of pain relievers.
Treatment Guidelines for Low Back Pain
A Patient’s Guide to Treatment Guidelines for Low Back Pain
Introduction
In the United States low back pain is ranked number five among the most common reasons for physician office visits. Of the patients who get medical care, they usually improve rapidly in the first month. However, up to one-third of patients report chronic back pain of at least moderate severity.
Many diagnostic tests and treatments have been tried for low back pain. Many things may be suggested, but have little evidence to show their worth. Diagnostic tests and treatments for low back pain can also be costly. In 1998, it is estimated that 26.3 million dollars were spent in the U.S. On health care for low back pain.
What to do about back pain can be confusing for both you and your provider. The American College of Physicians (ACP) and the American Pain Society (APS) recently had a panel review and analyzed available research on acute and chronic low back pain in adults.
The panel’s recommendations were considered proven only when they were supported by at least fair-quality evidence. They also had to have at least moderate benefits. Some were considered proven even with small benefits if there were no significant harms, costs, or burdens.
This guide will give you a general overview of the newly recommended
guidelines for the evaluation, diagnosis, and treatment of acute and chronic low back pain in adults.
This guide will help you understand
- how your doctor will evaluate your low back pain
- what diagnostic tests are recommended
- what treatment options are recommended based on evidence
Recommendation 1:
Clinicians should conduct a focused history and physical examination to help place patients with low back pain into 1 of 3 broad categories: nonspecific low back pain, back pain potentially associated with radiculopathy or spinal stenosis, or back pain potentially associated with another specific spinal cause. The history should include assessment of psychosocial risk factors, which predict risk for chronic disabling back pain (strong recommendation, moderate-quality evidence).1
Your doctor will want to do a history and physical examination to determine if there is a specific reason for your low back pain. It is important for your doctor to determine if there is neurologic (nerve) involvement. Your back pain can then be placed into one of three categories:
- non-specific back pain
- back pain with radiculopathy (leg pain)
- back pain from another specific source (fracture, infection, tumor, etc.)
The most common category is non-specific back pain. This means that the cause of the pain is unknown. More than 85% of patients evaluated in the primary care setting with low back pain have non-specific low back pain. This means there are no findings of a specific disease or spinal abnormality.
Another category is back pain with leg pain. Leg pain is called radiculopathy or sciatica. This may be caused by a problem with a disc between the bones of the spine. Discs may be torn (annular tear), bulged (protruded), or ruptured (herniated). Leg pain can also be caused by stenosis. Stenosis happens when the hollowed out portion of the bones of the spine become narrowed. The spinal cord lies in the hollowed out portion. When it becomes narrow, the spinal cord can become pinched. Stenosis can also happen when there is narrowing of the opening for the nerve root. The nerve root branches off the spinal cord.
Other specific spinal causes of low back pain include fracture, infection, tumor, cancer, and inflammatory arthritis.
Spinal cord and nerve function can be evaluated in several ways. Straight leg raise (SLR) test is when your doctor lifts your leg up while the knee is kept straight. This can be useful in diagnosing a herniated disc. Your doctor will want to check the strength of various muscles in the legs. Reflexes at the knees and ankles should be evaluated also. Sensation of the leg also evaluates nerve function.
Other signs that there may be a neurological problem include loss of bowel or bladder function.
Your doctor will ask questions about the possibility of low back pain that comes from problems outside the back. Sometimes pain is from the pancreas, kidneys, or bulging of the large blood vessel in the abdomen called the aorta. Your doctor will also want to know about risk factors for cancer and infection.
Your doctor will ask about any problems with your mood, stress, or problems at home or on the job. Psychosocial factors are known to make your back pain worse, or interfere with your back pain getting better. These include depression, passive coping strategies, job dissatisfaction, disputed compensation claims, and being overly focused on physical symptoms. These problems can predict the course of low back pain even more so than findings on the physical exam, or the severity of your pain.
Recommendation 2:
Clinicians should not routinely obtain imaging or other diagnostic tests in patients with nonspecific low back pain (strong recommendation, moderate-quality evidence).1
There is no evidence that routine plain x-rays in patients with nonspecific low back pain improve patient outcomes. They subject you to a significant amount of radiation. The amount of radiation to reproductive (sperm and egg) cells from two views of the lumbar spine is equivalent to being exposed to a daily chest x-ray for more than one year.
Plain x-rays are recommended when there is the possibility of compression fracture of the vertebra bone. High-risk patients are those with a history of osteoporosis or steroid use.
Your doctor may want you to have imaging when nonspecific low back pain (without symptoms of radiculopathy or spinal stenosis) becomes persistent (lasting more than four to eight weeks). There is no optimal evidence to make a recommendation as to which imaging study is most useful in this case.
Recommendation 3:
Clinicians should perform diagnostic imaging and testing for patients with low back pain when severe or progressive neurologic deficits are present or when serious underlying conditions are suspected on the basis of history and physical examination (strong recommendation, moderate-quality evidence).1
Neurologic deficits or the suspicion of a serious underlying condition such as cancer or infection merit a prompt work-up with Magnetic Resonance Imaging (MRI) or Computed Tomography (CT). Delayed diagnosis is linked to worse outcomes.
MRI allows your doctor to look at slices of the area in question. The MRI machine uses magnetic waves, not x-rays to show the soft tissues of the body. This includes the spinal cord, nerves, and discs. It can also evaluate spinal bones. The test may require that a dye be injected intravenously (through a vein).
CT scans are a form of x-ray. MRIs are generally preferred over CTs since it does not use radiation.
If you have risk factors for cancer, the recommendations are for either x-rays, blood work to measure erythrocyte sedimentation rate (ESR), or an MRI.
Recommendation 4:
Clinicians should evaluate patients with persistent low back pain and signs or symptoms of radiculopathy or spinal stenosis with MRI (preferred) or CT only if they are potential candidates for surgery or epidural steroid injection (strong recommendation, moderate-quality evidence).1
Most patients with lumbar disc herniations with radiculopathy improve with noninvasive therapy (treatments other than spinal injections or surgery) within the first four weeks.
If symptoms of radiculopathy become persistent after noninvasive therapies, the panel recommends surgical removal of the disc or epidural steroid injections as possible treatment options. Surgery is also a treatment option for spinal stenosis with persistent symptoms.
Recommendation 5:
Clinicians should provide patients with evidence-based information on low back pain with regard to their expected course, advise patients to remain active, and provide information about effective self-care options (strong recommendation, moderate-quality evidence).1
Your doctor should inform you that an acute episode of low back pain with or without radiculopathy or sciatica should more than likely improve in the first month.
The evidence shows that staying active is more effective than resting in bed. Return to normal activities as soon as possible should be encouraged. Self-care education books are inexpensive and have shown to be helpful. Their benefits are similar to costlier therapies such as supervised exercise, acupuncture, massage, and spinal manipulation.
The panel authors did not find sufficient evidence to guide specific recommendations about modified work on the job. Factors to consider are your age, general health, and physical demands of your required job tasks.
Use of heating pads may provide short-term relief of acute low back pain. There is not adequate evidence to recommend lumbar supports and cold packs.
Recommendation 6:
For patients with low back pain, clinicians should consider the use of medications with proven benefits in conjunction with back care information and self-care. Clinicians should assess severity of baseline pain and functional deficits, potential benefits, risks, and relative lack of long-term efficacy and safety data before initiating therapy (strong recommendation, moderate-quality evidence). For most patients, first-line medication options are acetaminophen or nonsteroidal anti-inflammatory drugs (NSAIDs).1
Medications from several classes have been shown to have moderate, mostly short-term benefits for patients with low back pain.
Acetaminophen (Tylenol®) is a slightly weaker pain medication than non-steroidal anti-inflammatories (NSAIDs). However, acetaminophen is generally safer and less costly. Acetaminophen can cause liver enzyme elevations at dosages of 4 g (4,000 mg)/day even in healthy adults. The clinical significance of the liver enzyme elevation is uncertain.
NSAIDs can be selective, or non-selective. Advil® and Motrin® (ibuprofen); and Aleve® (naproxen) are examples of over-the-counter non-selective NSAIDs. Celebrex® is the only selective NSAID available in the United States. Nonselective NSAIDs, while more effective than acetaminophen, are known to cause stomach and kidney problems. Selective NSAIDs such as Celebrex® and most non-selective NSAIDS also increase risk for heart attack. The lowest effective doses for the shortest periods necessary are recommended. If you benefit from nonselective NSAIDs, taking a medication to protect the stomach lining may be beneficial and more cost-effective than a selective NSAID. It was also recommended that doctors remain alert for new evidence about the safety of NSAIDs. There is not enough evidence to recommend for or against aspirin to treat low back pain.
When used carefully opioid analgesics (Tramadol) are an option in the management of acute or chronic severe, disabling low back pain. Potential risks such as addiction and abuse should be considered before starting them. There is not enough evidence to recommend one opioid over another.
Skeletal muscle relaxants may provide short term relief of acute low back pain. There is no convincing evidence that skeletal muscle relaxants differ in effectiveness or safety. Sedation can be a problem with any of the muscle relaxants.
Tricyclic antidepressants such as Pamelor® have demonstrated effectiveness in the management of chronic low back pain. Selective serotonin reuptake inhibitors (SSRIs) such as Prozac®, Zoloft®, Celexa® and Lexapro®, and trazodone have not shown that they are effective for low back pain. Serotonin-norepinephrine reuptake inhibitors (SNRIs) have not yet been evaluated for low back pain. Since depression is common in patients with chronic low back pain, it should be properly treated.
Small, short-term benefits for the treatment of leg pain or radiculopathy have been found with gabapentin (Neurontin®). There is not adequate evidence to recommend for or against other similar drugs for radiculopathy.
Benzodiazepines such as Valium® (diazepam) provide short-term pain relief for acute or chronic low back pain. However, they can be abused, cause addiction, and require more of them to get the same result. When benzodiazepines are used, a time-limited course is recommended.
Herbal therapies including devil’s claw, willow bark, and capsicum seem to be safe options for acute exacerbations of chronic low back pain.
Systemic corticosteroids have not been shown to be helpful in the treatment of low back pain with or without sciatica.
Overall, evidence is limited on the benefits and risks when medications are used long-term for low back pain.
Recommendation 7:
For patients who do not improve with self-care options, clinicians should consider the addition of nonpharmacologic therapy with proven benefits for acute low back pain, spinal manipulation; for chronic or subacute low back pain, intensive interdisciplinary rehabilitation, exercise therapy, acupuncture, massage therapy, spinal manipulation, yoga, cognitive-behavioral therapy, or progressive relaxation (weak recommendation, moderate-quality evidence).1
Spinal manipulation may provide small to moderate short-term benefits for acute low back pain. Supervised exercise therapy, home exercise regimens, and other non-medication treatments have not been proven to be effective for acute low back pain.
For subacute low back pain (lasting four to eight weeks), intensive interdisciplinary rehabilitation is moderately effective. This usually includes the services of a physician, psychologist, physical therapist, social worker, or vocational counselor. Active physical therapy to restore function and a form of psychological treatment called cognitive-behavioral therapy (CBT) are shown to reduce time off work due to low back pain.
For chronic low back pain there are non-medication treatments with fair to good supporting evidence and moderate benefit. These include acupuncture, massage therapy, and Viniyoga-style yoga. Exercise therapy has also shown fair to good supporting evidence. This includes individualized, supervised stretching, and strengthening therapy. Cognitive-behavioral therapy (CBT) or progressive relaxation, spinal manipulation, and intensive interdisciplinary rehabilitation have also shown moderate benefit. Short-term benefits may be obtained with back schools, but the evidence is inconsistent.
Transcutaneous electrical nerve stimulation (TENS) and intermittent or continuous traction have not been proven effective for chronic low back pain. There is insufficient evidence to recommend interferential therapy, low-level laser, shortwave diathermy, or ultrasound for chronic low back pain.
Lastly, the panel recommends that patient expectations of benefit from a treatment be considered when choosing therapies. They found that this seems to positively influence outcomes.
1. Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low back pain: A joint clinical practice guideline from the American College of Physicians and the American Pain Society. Annals of Internal Medicine 2007. Vol. 147, No. 7. Pp. 478–491.
Sacral Insufficiency Fractures
A Patient’s Guide to Sacral Insufficiency Fractures
Introduction
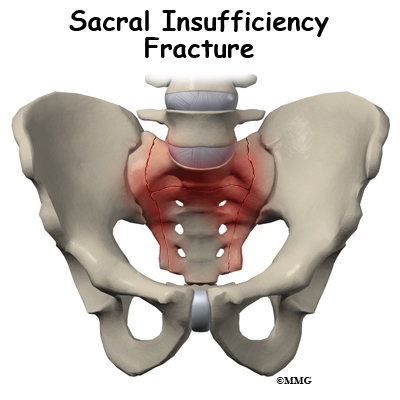
The sacrum is a wedge shaped bone that makes up part of the pelvis. It transmits the weight of the body to the pelvic girdle. As the name suggests, sacral insufficiency fractures occur when the quality of the sacral bone has become insufficient to handle the stress of weight bearing. The bone has lost some of its supporting structure and has become weak. Since this is usually because of osteoporosis, sacral insufficiency fractures occur most often in older women.
This guide will help you understand
- what parts make up the sacrum
- what causes this condition
- how doctors diagnose this condition
- what treatment options are available
Anatomy
What makes up the sacrum?
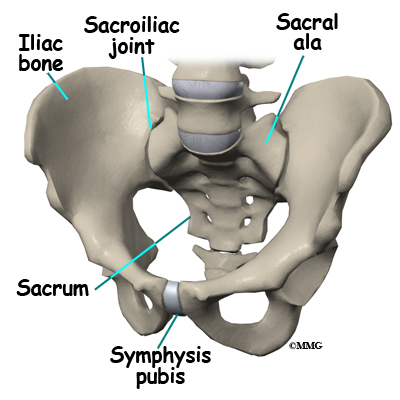
The sacrum is the triangular bone just below the lumbar spine. The sacrum has five segments fused together into one large bone. The coccyx or tailbone attaches to the bottom of the sacrum.
The sacrum forms the base of the spine and the center of the pelvis. The sacrum transmits the weight of the body to the pelvic girdle. It is shorter and wider in the female than in the male. Its name means “sacred bone”.
At the top of the sacrum there are wings from each side called the sacral ala. At the ala, the sacrum fits between the two halves of the pelvis. These pelvic bones are called the iliac bones. This is where the sacroiliac joints are formed. Most everyone has two dimples in their low back where the sacroiliac joints form. These three bones of the pelvis, the sacrum and the two iliac bones, make a ring.
Each of the iliac bones has projections called the pubic rami. They meet together in the front of the pelvis, forming a joint called the symphysis pubis. The iliac bones also contain the cup or socket for the hip joint.
Nerves that leave the spine in the area of the sacrum help control the bowels and bladder and provide sensation to the crotch area.
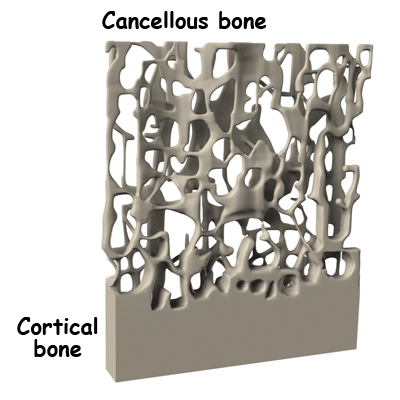
There are three types of bone, woven bone, cortical bone, and cancellous bone. In adults, woven bone is found where there is a broken bone that is healing (callus formation). It can also be found with hyperparathyroidism and Paget’s disease. It is composed of randomly arranged collagen strands. It is normally remodeled by the body and replaced with cortical or cancellous bone.
Cortical bone is called compact or lamellar bone. It forms the inside and outside tables of flat bones and the outside surfaces of long bones. It is dense and makes up 80 percent of our bone mass. The radius (wrist bone), skull, and long bones are made of cortical bone.
Cancellous bone is also called trabecular bone. It lies between the cortical bone surfaces. It is the inner supporting structure and is spongy. It makes up 20 percent of our bone mass. Normal cancellous bone is always undergoing remodeling on the inside surfaces of bone. Cancellous bone is found in the hip, spine, and femur.
The three main cells that form and shape bones are osteoblasts, osteocytes, and osteoclasts. Osteoblasts are bone-forming cells. When calcium is deposited in the cells, they make bones strong and hard. Osteocytes are mature osteoblasts trapped within the bone. Osteoclasts are bone-resorbing cells. They dissolve bone surfaces by releasing a chemical called an enzyme. Their activity is in part controlled by hormones in the body.
It is normal for bones to have mini fractures from everyday wear and tear. They are healed by ongoing bone remodeling. Bone remodeling occurs in 120 day cycles. Normal bone has a balance of clearing away old bone and formation of new bone. Osteoclasts resorb or clear away the damaged bone for the first 20 days. Bone is then formed by osteoblasts over the last 100 days.
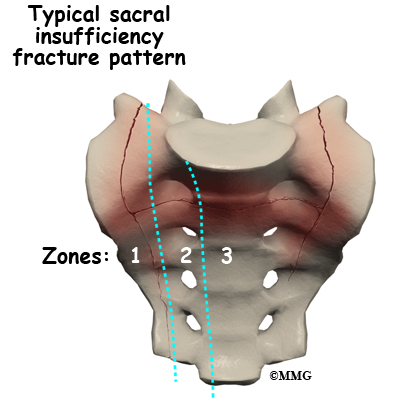
Sacral insufficiency fractures usually are parallel to the spine. They are most often in the ala, just beside the sacroiliac joint. At times there is also a transverse fracture that connects insufficiency fractures when they occur on both sides of the sacrum. The fracture lines then create an “H” pattern. Sacral fractures are classified into three zones, zone 1, zone 2, and zone 3. If the fracture involves just the ala, there is usually not a risk for nerve damage.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Causes
What causes sacral insufficiency fractures ?
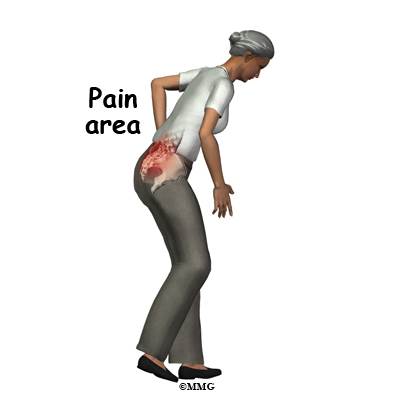
A physician named Lourie first described sacral insufficiency fractures in 1982. These fractures can cause severe pain in the buttock, back, hip, groin, and/or pelvis. Walking is typically slow and painful. Many daily activities become painful, difficult, and in some cases impossible.
Sacral insufficiency fractures occur when the quality of the sacral bone has become insufficient to handle the stress of weight bearing. The bone has lost some of its supporting structure and has become weak.
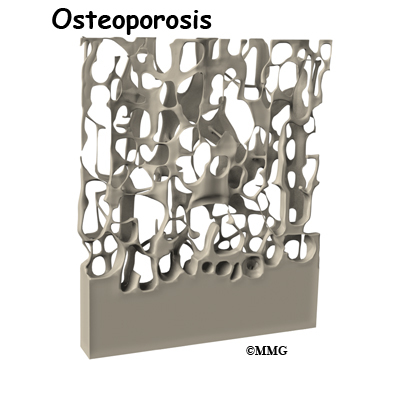
Osteoporosis is the leading cause of sacral insufficiency fractures. Osteoporosis is defined as low bone mass (weight). There is a decrease in bone tissue and minerals such as calcium. This can make the bones fragile. This means they can break more easily. Bone mineral density is measured by a DEXA scan. DEXA involves scanning the lumbar spine, the hip, and sometimes, the wrist. Osteoporosis affects 25 million people in the United States. Of these, 80 percent are females.
Other risk factors that can weaken bone include radiation to the pelvis, steroid use, rheumatoid arthritis, hyperparathyroidism, anorexia nervosa, liver transplantation, osteopenia, Paget’s disease, hip joint replacement, and lumbosacral fusion. Sacral insufficiency fractures can also occur in pregnant or breastfeeding women due to temporary osteoporosis.

Sacral insufficiency fractures can occur spontaneously, meaning there does not need to be any trauma such as a fall. The fracture can just simply happen when the bone becomes too weak to handle the stress of weight bearing. When the sacrum is fractured, 60 percent of the time the bone in front of the pelvis will also fracture. This bone is called the pubic ramus.
Symptoms
What does a sacral insufficiency fracture feel like ?
Unfortunately, sacral insufficiency fractures are often an unsuspected and undiagnosed cause of low back pain in elderly women. It was not until 1982 that they were described by a physician named Lourie.
Symptoms can include severe pain in the buttock, back, hip, groin, and/or pelvis. If the pubic ramus has fractured, there may be pain in the front of the pelvis. Walking is typically slow and painful. It can be difficult to do other necessary activities. Your back or pelvis may be tender to touch. You may find that you have limited range of motion of your low back.
Rarely there is nerve damage with sacral insufficiency fractures. When nerve damage does occur, the symptoms are usually problems with bowel or bladder function, or decreased sensation or strength of the leg(s).
Diagnosis
How do doctors diagnose the problem?
Your doctor will want to ask questions about your general health, what your symptoms feel like, and if there was any trauma that could have caused your symptoms.
Your doctor will want to perform a physical exam. This will likely include checking your nerve and spinal cord function, checking your range of motion, and feeling or tapping your back and pelvis to check for tenderness.
Your doctor will want you to have imaging of your pelvis. Plain X-rays are often negative. However, a fracture will be seen on bone scan, Computed Tomography (CT), or Magnetic Resonance Imaging (MRI).
Your doctor may order a bone scan with technetium-99m medronate ethylene diphosphonate (MDP). The MDP is injected into your vein. This should be performed after a minimum of 48 to 72 hours after symptoms begin. Where there is a fracture, the MDP will be concentrated. Uptake patterns on the scan may include the “H”-shape, also called the Honda sign when there is a sacral insufficiency fracture.
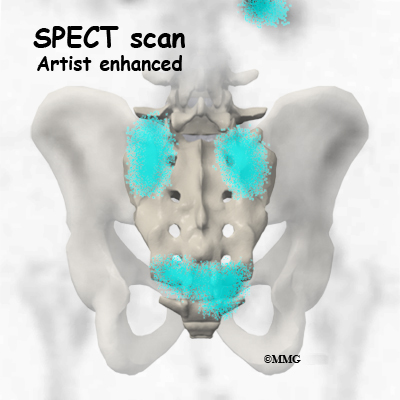
Single Photon Emission Computed Tomography (SPECT) is a new, advanced diagnostic nuclear medicine procedure that uses the emission of a radioisotope that is carried in the blood to the tissues. SPECT imaging is often added to provide information that is not available on routine bone scan images. It provides three-dimensional (3-D) views of the area examined. Following a bone scan you will remain on the exam table and the camera will rotate around the table while it takes pictures. SPECT imaging adds 30 to 60 minutes to the time of the nuclear scan. Sedation may be needed.
CT scan may be used to confirm and complement a positive bone scan. The CT scan uses special Xrays.
MRI is the radiological examination of choice by some doctors. Bone marrow edema on an MRI suggests a fracture. The MRI machine uses magnetic waves, not X-rays to show the bone and soft tissues.
Your doctor may request that you give samples of blood for the laboratory. This is to see if there could be another cause for osteoporosis that can be treated.
Treatment
What treatment options are available?
Most of the time treatment for sacral insufficiency fractures is non-surgical.
Nonsurgical Treatment
Treatment consists of rest, pain medications, and gradual walking with a walker or crutches. Improvement of symptoms may begin after one to two weeks of treatment. Most people are pain free in six to 12 months. Complete healing may occur after nine months. Most patients should have a full recovery.
Water exercise may be recommended to allow movement.
Bracing with a corset is sometimes helpful.
Medications that are used to help the fracture heal include calcium (1200-1500mg) and Vitamin D (400-800 IU). Bisphoshonates such as Actonel, Fosamax and Boniva are used to treat osteoporosis. Calcitonin is also used to help with pain and healing of the bone when broken. Parathyroid hormone (PTH) replacement can also be beneficial. It increases both bone resorption and bone formation. Bone mineral density is increased, making the bone stronger.
For pain, narcotics or opioids can be helpful. Some doctors feel that nonsteroidal anti-inflammatories (NSAID) such as Aleve or Ibuprofen should not be used for at least three to four weeks after a new fracture. Some studies have shown that they can slow fracture healing.
Your doctor may want you to have physical therapy to help with your pain. Heat, gentle massage, and electrical stimulation, or TENS units may improve pain.
Surgery
Surgical treatment is rare with sacral insufficiency fractures. A newer treatment that shows some promise in relieving pain and allowing more normal activity sooner is called a sacroplasty.
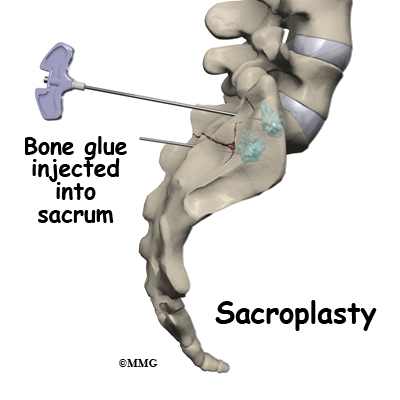
During sacroplasty, a bone glue called polymethylmethacrylate (PMMA) is injected into the fracture. Serious complications can occur if it is not performed correctly.
Sacroplasty may be considered in those with a severe decrease in functional ability and quality of life. It may provide faster relief of pain than typical conservative care. It is usually done in a surgery suite.
The area that is to be injected is cleaned and sterilized. This helps to decrease the possibility of an infection. A needle is placed in the area over the fracture. This is monitored with an X-ray machine. Bone glue is then injected and hardens rather quickly. This stabilizes the fracture. You are usually allowed to go home the same day.
If there are neurological symptoms from the sacral fracture, The sacrum may need to be stabilized. Hardware such as screws and plates may be used.
Rehabilitation
What should I expect after treatment?
Nonsurgical Rehabilitation
Previously, bedrest was the recommended treatment for sacral insufficiency fractures. There are many complications of prolonged bedrest, especially in the elderly.
Medical management presently allows limited weight bearing. This can be tolerated with a wheeled walker or crutches in most cases. Limited weight bearing actually helps to stimulate new bone growth.
In six to nine months, you should be able to return to your previous activity level.
If you have a sacroplasty, the fracture will be considered healed much more quickly. This allows you to return to your previous activity level sooner also. Your doctor will likely repeat imaging studies to check the progress of the healing fracture(s).
Treating osteoporosis is crucial in an attempt to decrease the risk of another insufficiency fracture. Your doctor will likely recommend additional calcium, vitamin D. A prescription medication to help prevent mineral loss from your bones is also commonly used. Regular follow up with your doctor is important. DEXA scans are usually repeated to ensure that the treatments for your osteoporosis are working.
Weight bearing activities such as walking, and lifting light weights can be helpful. Avoiding excessive caffeine, alcohol, and smoking is important.
After Surgery
You will likely have to remain non-weight bearing for a period of time before being allowed to walk with a walker or crutches. You will need assistance for daily activities initially. This may mean that you will have to have live-in help, or stay in an extended care facility or nursing home.
Once allowed, your surgeon may want a physical therapist to help with walking and maintaining strength. Your surgeon may want an occupational therapist to help you with equipment that may be helpful, showering, dressing, and other daily activities.
Your surgeon will want you to follow up with him or her on a regular basis to check on how the fracture is healing. Imaging studies will be repeated. Healing should occur in six to 12 months. If the fracture heals properly, you should be able to return to your usual activities.
Treating osteoporosis is crucial in an attempt to decrease the risk of another insufficiency fracture. Your surgeon will likely recommend additional calcium, vitamin D. A prescription medication to help prevent mineral loss from your bones is also commonly used. Regular follow up with your doctor is important. DEXA scans are usually repeated to ensure that the treatments for your osteoporosis are working.
When allowed, weight bearing activities such as walking, and lifting light weights can help keep your bones strong. Avoiding too much caffeine, alcohol, and smoking is important.
Lumbar Artificial Disc Replacement
A Patient’s Guide to Lumbar Artificial Disc Replacement
Introduction

Artificial disc replacement (ADR) is a device or implant used to replace a diseased or damaged intervertebral disc. After removing what’s left of the worn out disc, the ADR is inserted in the space between two lumbar vertebrae. The goal is to replace the diseased or damaged disc while keeping your normal spinal motion. Artificial disc surgery is relatively new in the United States but has been used in Europe for many years. In the U.S., the first lumbar artificial disc surgery was done in clinical trials in October 2001. The Federal Drug Administration (FDA) approved the use of the lumbar ADRs in October 2004.
This guide will help you understand:
- what parts of the spine are involved
- what your surgeon hopes to achieve
- who can benefit from this procedure
- what happens during the procedure
- what to expect as you recover
Anatomy
What parts of the spine are involved?
The human spine is made up of 24 spinal bones called vertebrae. Vertebrae are stacked on top of one another to form the spinal column. The spinal column gives the body its form. It is the body’s main upright support. The section of the spine in the lower back is known as the lumbar spine. Lumbar disc replacement typically occurs in the lumbar spine (from L4-S1).
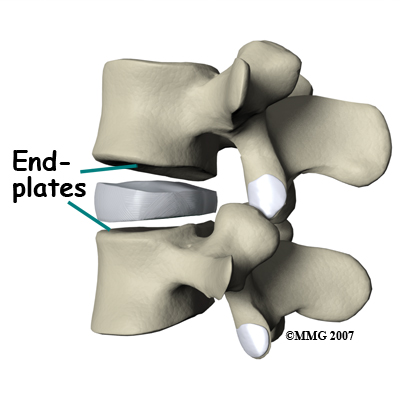
An intervertebral disc sits between each pair of vertebrae. The disc normally works like a shock absorber. It protects the spine against the daily pull of gravity. It also protects the spine during strenuous activities that put strong force on the spine, such as jumping, running, and lifting.
An intervertebral disc is made of two parts. The center, called the nucleus is spongy. It provides most of the disc’s ability to absorb shock. The nucleus is held in place by the annulus, a series of strong ligament rings surrounding it. Ligaments are connective tissues that attach bones to other bones.
Between the vertebrae of each spinal segment are two facet joints. The facet joints are located on the back of the spinal column. There are two facet joints between each pair of vertebrae, one on each side of the spine. A facet joint is made of small, bony knobs that line up along the back of the spine. Where these knobs meet, they form a joint that connects the two vertebrae. The alignment of the facet joints of the lumbar spine allows freedom of movement as you bend forward and back.
From the side, the spine forms three curves. The neck, called the cervical spine, curves slightly inward. The middle back, or thoracic spine, curves outward. The outward curve of the thoracic spine is called kyphosis. The low back, also called the lumbar spine, curves slightly inward. An inward curve of the spine is called lordosis.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Rationale
What does the surgeon hope to achieve?
Disc replacement surgery is done to stop the symptoms of degenerative disc disease. Discs wear out or degenerate as a natural part of aging and from stress and strain on the spine. Eventually, the problem disc collapses, which causes the vertebra above to sink toward the one below. This loss of disc height affects nearby structures – especially the facet joints.
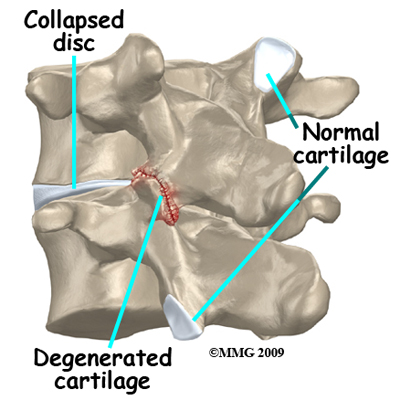
When the disc collapses it no longer supports its share of the load in the spine. The facet joints of the spine begin to support more of the force that is transmitted between each vertebra. This increases the wear and tear on the articular cartilage that covers the surface of the joints. The articular cartilage is the smooth, slippery surface that covers the surface of the bone in any joint in the body. Articular cartilage is tough, but it does not tolerate abnormal pressure well for long. When damaged, articular cartilage does not have the ability to heal. This wear and tear is what is commonly referred to as arthritis.
Shrinking disc height also reduces the size of the neural foramina, the openings between each vertebral pair where the nerve roots leave the spinal column. The arthritis also results in the development of bone spurs that may protrude into these openings further narrowing the space that the nerves have to exit the spinal canal. The nerve roots can end up getting squeezed where they pass through the neural foramina.
Replacing the damaged disc with an artificial disc, or implant, called a prosthesis can restore the normal distance between the two vertebrae. The artificial disc sits between the two vertebrae and distracts or “jacks up” the upper vertebra. Enlarging the disc space relieves pressure on the facet joints. It also opens up the space around the spinal nerve roots where they pass through the neural foramina.
Another benefit of the artificial disc replacement is that it mimics a healthy disc. Natural motion is preserved in the spine where the new disc is implanted. And it helps maintain stability in the spinal joints above and below it.
Who can benefit from this procedure?
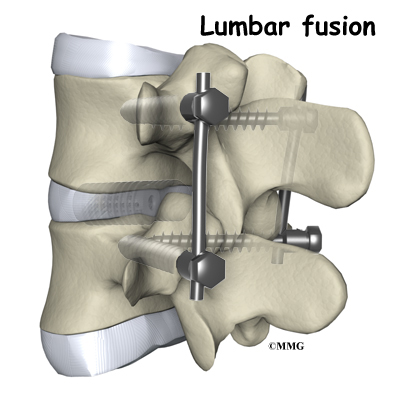
For many years, the standard of care for chronic pain from a degenerated disc has been spinal fusion surgery. Bone graft donated by a bone bank or taken from your pelvic bone is used to fuse two or more vertebral bones together. The spine is stabilized but you will lose motion at that level. The increased stress on the next lumbar vertebra can cause problems later.
The artificial disc replacement is used to reduce or eliminate the pain while still allowing motion. One advantage of the artificial disc is that it may also prevent premature breakdown of adjacent levels of the lumbar spine.
You may be a good candidate for a lumbar artificial disc replacement if you have chronic pain and disability from lumbar disc degeneration despite nonoperative treatment for at least six months. The artificial disc replacement provides an alternative to spinal fusion. The device helps restore the normal space between two vertebrae. You will still have movement at the level where the ADR is implanted.
Preparation
How should I prepare for surgery?
Knowing what to expect before and after surgery can help you plan for recovery at home. Once you and your surgeon have agreed that disc replacement surgery is indicated, certain preparations for the surgery are important.
You may need to visit your primary care physician or internal medicine specialist to obtain medical clearance for surgery. This will ensure that you are in the best medical condition prior to the surgery. A doctor who will be performing your anesthesia (an anesthesiologist) will evaluate and counsel you regarding anesthesia.
Certain factors put you at increased risk for problems during or after the operation. It’s best to reduce or eliminate as many of these risk factors as possible. For example, the use of alcohol or other drugs (including tobacco) can be major factors in how your body copes with anesthesia and the stress of surgery.
You should stop any anti-inflammatory medications 10 days before surgery. If you aren’t sure which medications this includes, ask your doctor. You should stop smoking or using tobacco as soon as possible but at least two weeks before surgery. This is very important to reduce complications from heart and lung problems. Smoking also decreases the success rate of spine surgery. Stopping smoking will increase your chance of a successful result.
You may need to donate one or two units of your own blood. This blood will be stored in the blood bank until surgery. If you need a transfusion either during or after your surgery you will receive your own blood back.
On the day of your surgery, you will probably be admitted to the hospital early in the morning. You shouldn’t eat or drink anything after midnight the night before. Let your surgeon know if you have diabetes and how you manage it (insulin pump, insulin injections, diet, exercise). Your need for insulin can change as a result of the stress of hospitalization and surgery. Even if you are tightly controlled now, you should monitor your glucose levels closely for at least a week before surgery and continue to do so for several weeks after surgery.
Surgical Procedure
What happens during the operation?
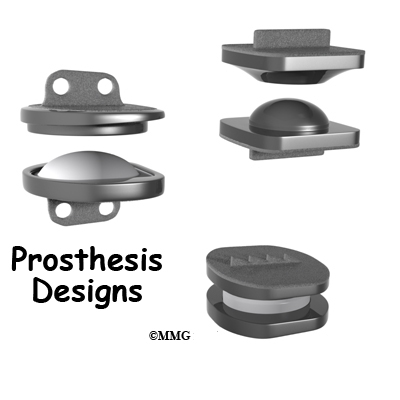
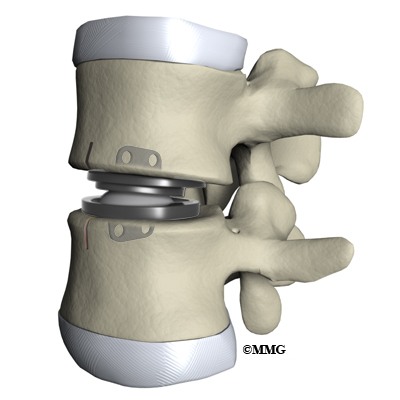
Before we describe the procedure, let’s look first at the artificial disc itself. The lumbar artificial disc has several different designs. They are made of metal, ceramic, and plastic. Some look like a sandwich with two endplates separated by a plastic spacer. The two endplates are made of cobalt chromium alloy, a safe material that has been used for many years in replacement joints for the hip and knee.
A plastic (polyethylene) core fits in between the two metal endplates. The core acts as a spacer and is shaped so that the endplates pivot in a way that imitates normal motion of the two vertebrae. There are small prongs or teeth on one side of each endplate. The teeth help anchor the endplate to the surface of the vertebral body.
Another way of anchoring the artificial disc replacement is the central keel or fin design. The implant is secured to the vertebral end plates by a thin, upright piece of metal that looks like the rudder on a boat or a shark’s fin.
Another artificial disc replacement design is a ball and socket articulation to allow for normal translation of motion at that segment. The implant may be made of titanium and polyurethane in a metal-on-plastic design. Some are made of stainless steel and are all metal-on-metal.
Inserted between two vertebrae, the prosthesis reestablishes the height between two vertebrae. As a result of enlarging the disc space, the nearby spinal ligaments are pulled tight, which helps hold the prosthesis in place. The prosthesis is further held in place by the normal pressure through the spine.
The lumbar artificial disc replacement comes in a variety of sizes and angles. There are constrained and unconstrained designs. The constrained devices provide a fixed center of rotation that doesn’t change. The unconstrained design allows the center of the implant to move forward and back slightly during lumbar motion. The surgeon can also choose an implant with the correct angle for each patient in order to build in the right amount of lordosis (spinal curvature).
The Operation
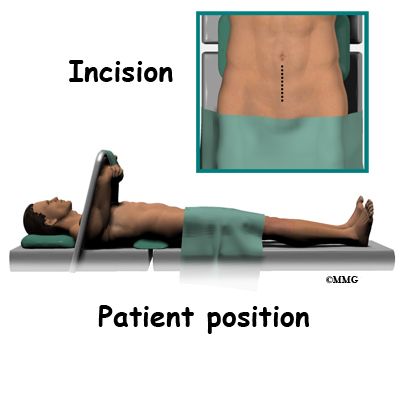
Lumbar ADR is done through the anterior ( front) of the spine. For your safety there are usually two surgeons present; your spine surgeon and a general or vascular surgeon.
The new system is placed in the spine through an incision though the abdomen or belly. Working from the front of the spine through the abdomen, the organs are carefully moved to one side. This makes it easier to see the front of the spine. The spine surgeon removes a large section from the middle of the damaged disc.

Next, the bones of the spine are spread apart to make more room to see and work inside the disc space. Using a surgical microscope, any remaining disc material toward the back of the disc is removed. The surgeon will also remove any disc fragments pressing against the nerve and shave off any osteophytes (bone spurs).
The disc space is distracted (jacked up) to its normal disc height. This step helps decompress or take pressure off the nerves. At this point, x-rays or a fluoroscope, is used to insert the artificial disc device into the prepared disc space. The fluoroscope is an x-ray machine that allows the surgeon to actually see an x-ray image while doing the procedure. Using a fluoroscope, the surgeon is able to see where the implant goes as it is inserted. This makes the procedure much safer and much more accurate.
Finally, moving the spine in various positions tests the prosthesis. An X-ray may
be taken to double check the location and fit of the new disc.
Complications
What might go wrong?
All types of spine surgery, including artificial disc replacement, have certain risks and benefits. Complications from any kind of surgery can also occur from anesthesia, infection, and development of blood clots (thrombophlebitis). Medical complications arising from spinal surgery are rare but could include stroke, heart attack, spinal cord or spinal nerve injury, pneumonia, or possibly death.
Your spine surgeon will discuss the most common complications with you. This document will help you prepare any questions you may have. It doesn’t provide a complete list of all the possible complications. Complications from the artificial disc replacement procedure are rare and are lower than for spinal fusion. Results continue to improve with advances in technology and better surgical techniques. The more common problems may include but are not limited to:
- problems with anesthesia
- thrombophlebitis (blood clots)
- infection
- nerve damage or paralysis
- spontaneous ankylosis (fusion)
- problems with the implant
- retrograde ejaculation (men only)
- ongoing pain
Anesthesia Complications
Problems can arise when the anesthesia given during surgery causes a reaction with other drugs you may be taking. In rare cases, a patient may have problems with the anesthesia itself. In addition, anesthesia can affect lung function because the lungs don’t expand as well while a person is under anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Thrombophlebitis (Blood Clots)
View animation of pulmonary embolism
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can happen after any operation. It occurs when blood in the large veins of the leg forms blood clots. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lung, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Most surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective is getting you moving as soon as possible after surgery. Two other commonly used preventative measures include
- pressure stockings to keep the blood in the legs moving
- medications that thin the blood and prevent blood clots from forming
Infection
Infection following spine surgery is rare but can be a very serious complication. Some infections may show up early, even before you leave the hospital. Infections on the skin’s surface usually go away with antibiotics. Deeper infections that spread into the bones and soft tissues of the spine are harder to treat. They may require additional surgery to treat the infected portion of the spine.
Nerve Damage or Paralysis
Any surgery that is done near the spinal canal can potentially cause injury to the spinal cord or spinal nerves. Injury can occur from bumping, stretching, or cutting the nerve tissue with a surgical instrument. Nerve involvement can cause nerve pain, muscle weakness, and a loss of sensation to the areas supplied by the nerve.
These symptoms are usually temporary and will gradually go away in one to three months’ time. Swelling around the nerve or the formation of scar tissue can also result in pressure or traction on the nerve. Scar tissue called fibrosis does not always resolve resulting in chronic pain and long-term weakness and sensory changes.
Spontaneous Ankylosis
Scientists aren’t sure why but sometimes the spine fuses itself, a process called spontaneous ankylosis. Loss of spinal motion is the main side effect of this problem. Bone may also form in the soft tissues around the vertebrae. For example, cartilage turns to bone or bone-like tissue. This process is called ossification. Ossification may or may not affect the implant or your final results in terms of motion or function.
Problems with the Implant
The prosthesis itself can sometimes be a source of complications. Although rare, the prosthesis can shift out of its normal position and even dislocate. If the implant migrates out of position, it can cause injury to the nearby tissues. A second surgery may be needed to align or replace the implant.
And similar to other types of joint replacements, the artificial disc may fail over time if the parts wear out. Your ADR is estimated to last 15 to 20 years. If the disc moves out of position or wears out, it can be removed. When surgery is done to take out the original prosthesis, a fusion surgery will most likely be recommended.
Subsidence is another possible problem. The implant actually sinks down into the vertebral body above or below it. This results in a loss of the normal disc height. Neurologic compression with neurologic symptoms can occur.
Over time, wear and tear just from the physical process of motion across a bearing surface can cause tiny bits of debris to flake off the implant. The body may react to these particles with an inflammatory response that can cause pain, implant loosening, and implant failure. So far, significant inflammatory reactions have not been reported for spinal ADRs.
Retrograde Ejaculation
Lumbar disc replacement surgery carries risks associated with operating from the front of the spine. In men, the anterior approach can also sometimes result in a complication called retrograde ejaculation.
Tiny nerves in front of the lower spine may be damaged during the anterior approach. If so, semen enters the bladder instead of going out through the urethra during ejaculation. Male patients planning a family might wish to consider donating sperm before surgery. Studies have not reported cases of sexual dysfunction but it is a potential risk.
Ongoing Pain
Not all patients get complete pain relief with this procedure. As with any surgery, patients should expect some pain afterward. If the pain continues or becomes unbearable, talk to your surgeon about treatments that can help control your pain.
After Surgery
What happens after surgery?
You may have immediate relief from your painful symptoms, but many people notice a gradual improvement over the next weeks to months. Many patients are able to reduce or eliminate the use of pain medication as well.
Your hospital stay will depend on how quickly you recover but most people are able to go home by the third day after surgery. You may require an extra day or two if for some reason you’re having extra pain or unexpected difficulty.
Most people recover quickly after the artificial disc procedure. You will be getting up out of bed and walking the same day as your surgery. You may even be able to get out of bed and walk within a few hours. Move carefully and comfortably, and avoid extending your back (bending backward). You probably won’t need a back brace or other support while the tissues are healing.
When you go home, you should be safe to sit, walk, drive, and ride a bike. Lifting anything more than eight to 10 pounds should be avoided for at least four weeks. To help you gauge what you can and can’t lift, keep in mind that a gallon of milk weighs about eight pounds.
Your surgeon will continue to follow-up with you. X-rays will be done from time to time to make sure the implant is still in its proper place. Your surgeon will let you know when you can return to work. Depending on the type of work you do, this should be in about two to four weeks. If your job requires moving and lifting heavy items, you may need a longer period of recovery. Your surgeon may give you the okay to do all your activities by the sixth week after surgery. You can expect to return to previous recreational activity by the end of three months.
Rehabilitation
What should I expect as I recover?
While you are in the hospital, a physical therapist will see you each day and advise you about ways to move. You’ll be shown how to do your daily activities without putting extra strain on your back.
Before you leave the hospital, you will have a home program of exercises and activities to help you regain motion and function. It’s important to continue with your walking program on a daily basis when you go home. Your goal should be to walk at least 30 minutes at a moderately brisk pace at least five days each week.
Your surgeon may prescribe outpatient physical therapy within one to two weeks after surgery. Plan on attending therapy two to three times each week for about four to six weeks. Active treatments are used to improve flexibility, strength, and endurance. Gentle stretching exercises for the back are commonly prescribed. You’ll begin a series of strengthening exercises to help tone and control the muscles that stabilize the trunk and back. It is also important to build strength in your legs. Endurance exercises may include treadmill walking, swimming, or stationary biking.
When your symptoms are under control and you’re comfortable doing your exercises, your formal therapy sessions will end. You’ll continue your exercises as part of a home program.
Summary
Artificial disc replacement may offer an alternative to spinal fusion for some patients who have chronic back pain from degenerative disc disease. While fusion stops pain by eliminating movement in the problem spinal segment, artificial disc replacement allows natural motion in the part of the spine where the disc is implanted. This is because the prosthesis is designed to restore normal motion and height between adjacent vertebrae. Artificial disc replacement allows for an early return to function.
The implant is designed to withstand bending, twisting, compression and repeated loads during movement. For active adults, successful disc replacement should endure years of high loads without mechanical failure.
Long-term studies to assess the safety and effectiveness of artificial disc replacements are ongoing. Researchers are looking at the impact of the ADR on other discs and on the bony structures of the spine. So far results show a low rate of complications. There have been no reports of death, significant infection, or major neurological problems. Patient satisfaction is good to excellent in most, but not all, cases.
Posterior Lumbar Interbody Fusion
Patient’s Guide to Posterior Lumbar Interbody Fusion
Introduction
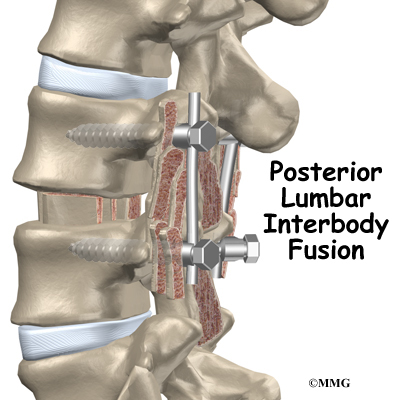
Posterior lumbar interbody fusion (PLIF) is a procedure used to treat problems such as disc degeneration, disc herniation, and spine instability. In this procedure, the surgeon works on the spine from the back (the posterior) and removes a spinal disc in the lower (lumbar) spine. The surgeon inserts bone graft material into the space between the two vertebrae where the disc was removed (the interbody space). The graft may be held in place with a special fusion cage. The goal of the procedure is to stimulate the vertebrae to grow together into one solid bone (known as a fusion). A fusion creates a rigid and immovable column of bone in the problem section of the spine.
This guide will help you understand
- what surgeons hope to achieve
- what happens during surgery
- what to expect as you recover
Anatomy
What parts of the spine and low back are involved?
This surgery is done through an incision in the low back. The incision reaches to the spinous processes, the bony projections off the back of the vertebrae. A large block of bone, called the vertebral body makes up the front section of each vertebra. The vertebral bodies are separated by a soft cushion
called an intervertebral disc.
On the back of the vertebral body, the lamina and pedicle bones form a protective ring around the spinal canal. The spinal nerves are enclosed in the spinal canal and exit through small openings on the sides of each vertebral pair, one on the left and one on the right. These passageways are called the neural foramina. (The term neural foramen describes a
single passageway).
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Rationale
What do surgeons hope to achieve?
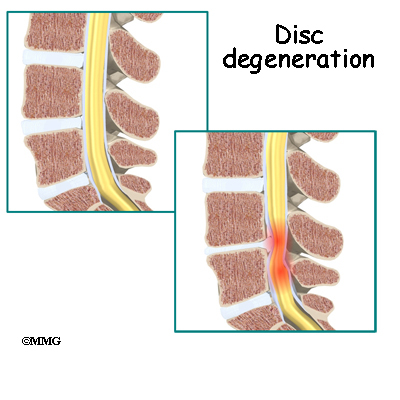
This procedure is often used to stop symptoms from lumbar disc disease. Discs degenerate, or wear out, as a natural part of aging and also from stress and strain on the back. Over time, the disc begins to collapse, and the space decreases between the vertebrae.
Related Document: A Patient’s Guide to Lumbar Degenerative Disc Disease
When this happens, the openings around the spinal nerves (the neural foramina) narrow and may put pressure on the nerves. The long ligaments in the spine slacken due to the collapse in vertebral height. These ligaments may even buckle and put pressure on the spinal nerves.
View animation of degeneration
Pain from disc degeneration can come from a tear in the outer portion of the disc, from chemical inflammation inside the disc, or from a herniated disc that pushes on a nearby spinal nerve. Mechanical pain can also occur from excess movement within the problem part of the spine.
Discectomy is the removal of the disc and any fragments between the vertebrae that are to be fused. Taking out the painful disc is intended to relieve symptoms. It also provides room for placing a graft that will allow the two vertebrae to fuse together.

Once the disc is removed, the surgeon spreads the bones of the spine apart slightly to make room to implant bone graft material. Bone graft is commonly taken from the rim of the pelvis and packed in a special case, called a fusion cage. Bone taken from your own body is called autograft. Bone substitutes are also being used and avoid the need for taking bone from your pelvis.
Another option is to use a wedge of hard, cortical bone taken from preserved human bone. This source of bone graft is called allograft. During the PLIF procedure, the cage or bone wedge is implanted into the interbody space. The PLIF method provides a large surface area for fusion to occur.
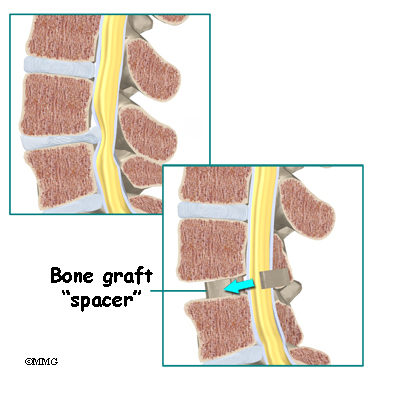
The graft creates a solid spacer to separate and hold the vertebrae apart. Enlarging the space between the vertebrae widens the opening of the neural foramina, taking pressure off the spinal nerves that pass through these openings. Also, the long ligaments that run up and down inside the spinal canal are pulled taut so they don’t buckle into the spinal canal.
View animation of creating a spacer
The surgeon also fixes the bones in place using pedicle screws. This instrumentation (or hardware, as it is sometimes called) holds the vertebrae together and prevents them from moving. The less motion there is between two bones trying to heal, the higher the chance they will successfully fuse. The use of instrumentation has increased the success rate of spinal fusions considerably.
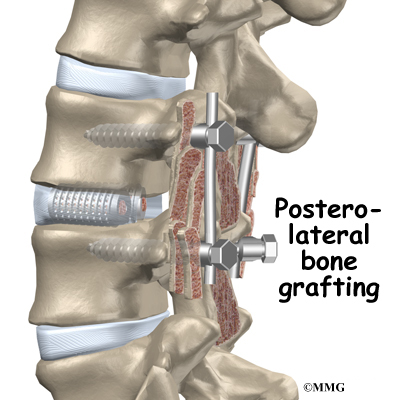
During the PLIF procedure, surgeons also commonly add bone graft material along the back sides of the spine. This step is called posterolateral bone grafting. When combined with instrumentation, this approach helps fuse a large surface area on the back (posterior column) of the spine.
In a successful fusion, the vertebrae that are fused together no longer move against one another. The fusion creates one solid bone. No movement happens within the bones that are fused. Instead, they move as one unit. This helps stop the mechanical pain that was coming from the moving parts of the back. Fusion also prevents additional wear and tear on the spinal segment that was fused. By fusing the bones together, surgeons hope to reduce future problems at the spinal segment.
Preparations
How will I prepare for surgery?
The decision to proceed with surgery must be made jointly by you and your surgeon. You should understand as much about the procedure as possible. If you have concerns or questions, you should talk to your surgeon.
Once you decide on surgery, your surgeon may suggest a complete physical examination by your regular doctor. This exam helps ensure that you are in the best possible condition to undergo the operation.
On the day of your surgery, you will probably be admitted to the hospital early in the morning. You shouldn’t eat or drink anything after midnight the night before.
Surgical Procedure
What happens during the operation?
Patients are given a general anesthesia to put them to sleep during most spine surgeries. As you sleep, your breathing may be assisted with a ventilator. A ventilator is a device that controls and monitors the flow of air to the lungs.
During surgery the patient usually kneels face down on a special operating table. The special table supports the patient so the abdomen is relaxed and free of pressure. This position reduces blood loss during surgery. It also gives the surgeon more room to work.
Two measurements are made before surgery begins. The first measurement ensures that the surgeon chooses a fusion cage or bone wedge that will fit inside the disc space. To correctly size the fusion cage or bone wedge, the surgeon uses an X-ray image to measure the disc space in a healthy disc, above or below the problem segment.
Second, to size the length of the pedicle screws, a CT scan is used to measure the length of the pedicle bone on the back of the vertebrae to be fused. The CT scan is a special type of X-ray that lets doctors see slices of bone tissue. The machine uses a computer and X-rays to create these slices.
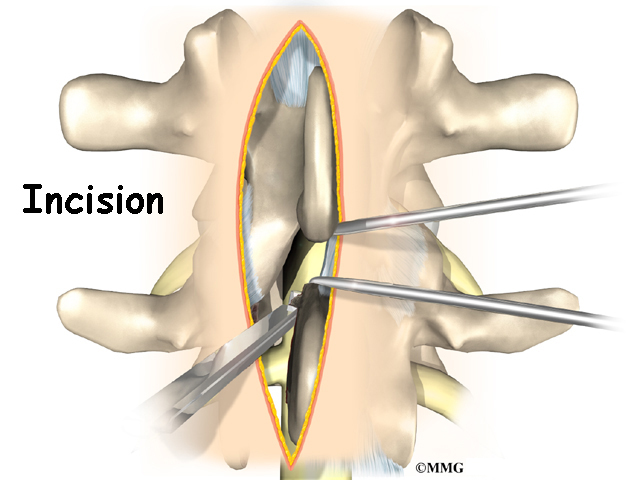
To begin the procedure, an incision is made down the middle of the low back. The tissues just under the skin are separated. Then the small muscles along the sides of the low back are moved aside, exposing the back of the spinal column. Next, the surgeon takes an X-ray to make sure that the procedure is being performed on the correct vertebrae.
The bone graft is prepared. When autograft (bone taken from your body) is used, the same incision made at the beginning of the surgery can be used. The surgeon reaches through the first incision and opens the tissues that cover the back of the pelvis. An osteotome is used to cut the surface of the pelvis bone. An instrument is used to gather a small amount of the pelvis bone. The graft material is prepared and will later be packed into the fusion cages. The tissues covering the pelvis bone are sutured.
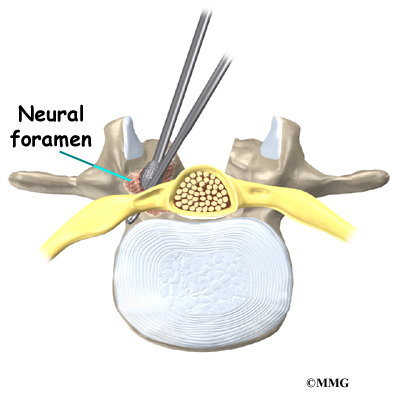
Then the surgeon prepares to implant bone graft into the space between the vertebral bodies. The surgeon removes the lamina bones that cover the back of the spinal canal. Next, the surgeon cuts a small opening in the ligamentum flavum, an elastic ligament separating the lamina bones and the spinal nerves. Removing the ligamentum flavum allows the surgeon to see inside the spinal canal. The nerves are checked for tension where they exit the spinal canal. If a nerve root is under tension, the surgeon enlarges the neural foramen, the opening where the nerve travels out of the spinal canal.
The surgeon locates the spot where the pedicle screws are to be placed. A fluoroscope is used to visualize the pedicle bones. A fluoroscope is a special type of X-ray that allows the surgeon to see an X-ray picture continuously on a TV screen. The surgeon uses the fluoroscope to guide one screw through the back of each pedicle, one on the left and one on the right.
The nerve roots inside the spinal canal are then pulled aside with a retractor so the problem disc can be examined. With the nerves held to the side, the surgeon is able to see the disc where it sits just in front of the spinal canal.
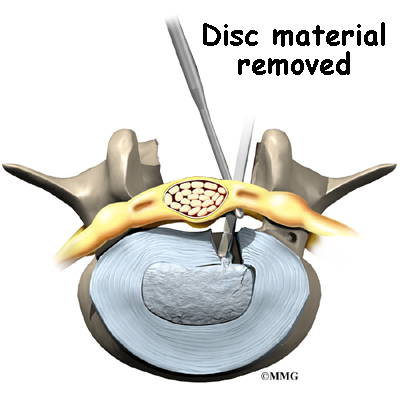
A hole is cut into the rim of the back of the disc. Forceps are placed inside the hole in order to clean out disc material within the disc. Reamers and scrapers are used to open up and remove additional disc material.
The surgeon prepares the disc space where the fusion cages or bone wedges are to be inserted. Special spreaders hold the two vertebral bodies apart. A layer of bone is shaved off the flat surfaces of the two vertebrae, causing the surfaces to bleed. Bleeding stimulates the bone graft to heal the bones together.
Adequate room is needed to get the bone graft implants through the spinal column and into the disc space. The nerve roots must be pulled as far to the side as possible to open up enough space.
With the disc space held apart by the spreaders, the surgeon has enough room to place the bone graft between the two vertebral bodies. For the fusion cage method, the surgeon packs two cages with bone taken from the pelvis bone or with a suitable bone substitute. Two cages are inserted, one on the left and one on the right. When allograft bone wedges are used, the surgeon inserts the wedges and aligns them within the disc space.
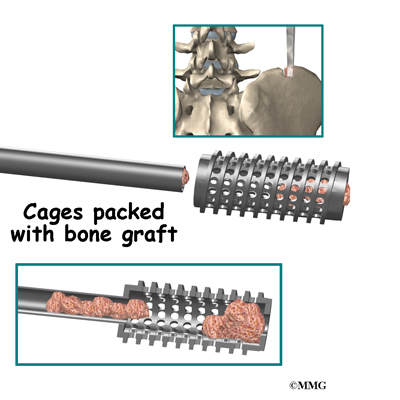
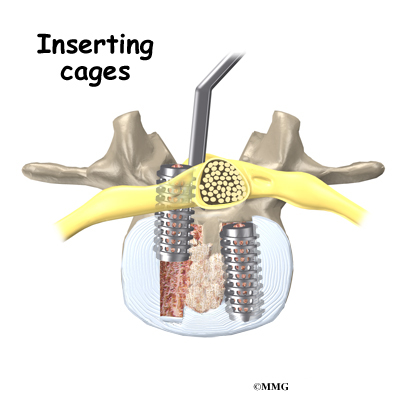
The surgeon uses a fluoroscope to check the position and fit of the graft.
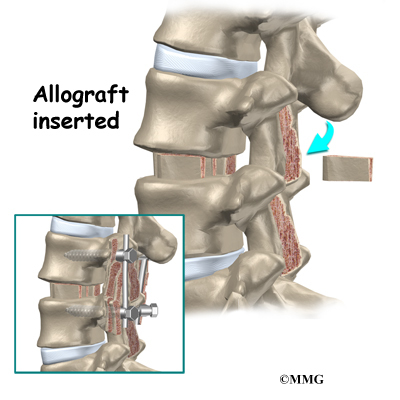
The spreaders used to hold the disc space apart are released. Then the doctor tests the graft by bending and turning the spine to make sure the graft is in the right spot and is locked in place.
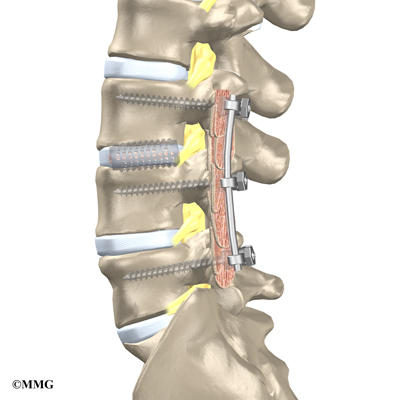
Some surgeons add strips of bone graft along the back of the vertebrae to be fused. This is called posterolateral fusion. The bones that project out from each side of the back of the spine are called transverse processes. The back surface of the transverse processes are shaved, causing the surfaces to bleed. Small strips of bone, usually taken from the pelvis bone at the beginning of the surgery, are placed over the transverse processes. The combination of this graft material with the pedicle screws helps hold the spine steady as the interbody fusion heals.
A drainage tube may be placed in the wound. The muscles and soft tissues are then put back in place. The skin is stitched together. The surgeon may place you in a rigid brace that straps across the chest, pelvis, and low back to support the spine while it heals.
Complications
What might go wrong?
As with all major surgical procedures, complications can occur. Some of the most common complications following PLIF include
- problems with anesthesia
- thrombophlebitis
- infection
- nerve damage
- problems with the implant or hardware
- nonunion
- ongoing pain
This is not intended to be a complete list of possible complications.
Problems with Anesthesia
Problems can arise when the anesthesia given during surgery causes a reaction with other drugs the patient is taking. In rare cases, a patient may have problems with the anesthesia itself. In addition, anesthesia can affect lung function because the lungs don’t expand as well while a person is under anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Thrombophlebitis (Blood Clots)
View animation of pulmonary embolism
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can happen after any operation. It occurs when the blood in the large veins of the leg forms blood clots. This may cause the leg to swell and become warm to the touch and painful. If the
blood clots in the veins break apart, they can travel to the lung, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Most surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective is getting you moving as soon as possible. Two other commonly used preventative measures include
- pressure stockings to keep the blood in the legs moving
- medications that thin the blood and prevent blood clots from forming
Infection
Infection following spine surgery is rare but can be a very serious complication. Some infections may show up early, even before you leave the hospital. Infections on the skin’s surface usually go away with antibiotics. Deeper infections that spread into the bones and soft tissues of the spine are harder to treat. They may require additional
surgery to treat the infected portion of the spine.
Nerve Damage

Any surgery that is done near the spinal canal can potentially cause injury to the spinal cord or spinal nerves. Injury can occur from bumping or cutting the nerve tissue with a surgical instrument, from swelling around the nerve, or from the formation of scar
tissue.
The nerve roots inside the spinal canal are especially at risk during the PLIF procedure. Retractors are used to hold the nerves aside and may cause muscle weakness and a loss of sensation to the areas supplied by an injured nerve. Pressure on the nerves that supply the bowels and bladder can cause incontinence. However, these types of nerve problems after PLIF usually go away soon after surgery.
Problems with the Implant or Hardware
Fusion surgery with cages requires bone grafting. The graft is commonly taken from the top rim of the pelvis (autograft). There is a risk of pain, infection, or weakness in the area where the graft is taken. These risks are avoided when a bone graft substitute is used in place of an autograft.
After the interbody implant is placed, the surgeon checks the position of the fusion cage or bone wedge before completing the surgery. However, the implant may shift slightly soon after surgery to the point that it is no longer able to hold the spine stable. If the implant migrates out of position, it can cause injury to the nearby tissues. A second surgery may be needed to align or replace the implant.
Hardware can also cause problems. Screws or pins may loosen and irritate the nearby soft tissues. Also, the metal plates can sometimes break. If this happens, the surgeon may suggest another surgery either to take out the hardware or to add more hardware to solve the problem.
Nonunion
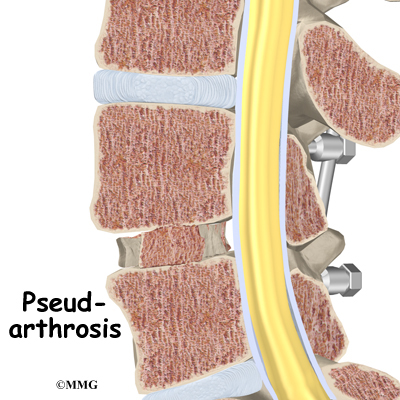
Sometimes the bones do not fuse as planned. This is called a nonunion, or pseudarthrosis. (The term pseudarthrosis means false joint.) When more than one level of the spine is fused at one time, there is a greater chance that nonunion will occur. (Fusion of more than one level means two or more consecutive discs are removed and replaced with bone graft.) If the joint motion from a nonunion continues to cause pain, the patient may need a second operation.
In the second procedure, the surgeon usually adds more bone graft. Additional instrumentation may also be needed to rigidly secure the bones so they will fuse together.
Ongoing Pain
PLIF is a complex surgery. Not all patients get complete pain relief with this procedure. As with any surgery, patients should expect some pain afterward. If the pain continues or becomes unbearable, talk to your surgeon about treatments that can help control your pain.
Afterward
What happens after surgery?
Patients are sometimes placed in a rigid body brace after surgery. The surgical drain is removed within one to two days.
Patients usually stay in the hospital after surgery for three to five days. During this time, patients work daily with a physical therapist. The therapist demonstrates safe ways to move, dress, and do activities without putting extra strain on the back. The therapist
may recommend that the patient use a walker for the first day or two. Before going home, patients are shown ways to help control pain and avoid problems.
Patients are able to return home when their medical condition is stable. However, they are usually required to keep their activities to a minimum in order to give the fusion time to begin healing. Patients are cautioned against bending, lifting, twisting, driving, and prolonged sitting for up to six weeks. Outpatient physical therapy is
usually started a minimum of six weeks after the date of surgery.
Rehabilitation
What should I expect as I recover?
Rehabilitation after PLIF can be a slow process. Many surgeons prescribe outpatient physical therapy beginning a minimum of six weeks after surgery. This delay is needed to make sure the graft has time to begin to fuse. You will probably need to attend therapy sessions for two to three months. You should expect full recovery to take up to eight months.
At first, treatments are used to help control pain and inflammation. Ice and electrical stimulation are commonly used to help with these goals. Your therapist may also use massage and other hands-on treatments to ease muscle spasm and pain.
Active treatments are slowly added. These include exercises for improving heart and lung function. Short, slow walks are generally safe to start with. Swimming and use of a stairclimbing machine are helpful in the later phases of treatment. Therapists also teach
specific exercises to help tone and control the muscles that stabilize the low back.

Your therapist also works with you on how to move and do activities. This form of treatment, called body mechanics, is used to help you develop new movement habits. This training helps you keep your back in safe positions as you go about your work and daily activities. Training includes positions you use when sitting, lying, standing, and walking. You’ll also work on safe body mechanics with lifting, carrying, pushing, and pulling.
As your condition improves, the therapist tailors your program to prepare you to go back to work. Some patients are not able to go back to a job that requires strenuous tasks. Your therapist may suggest changes in job tasks that enable you to go back to your previous job or to do alternate forms of work. You’ll learn to do these tasks in new ways that keep your back safe and free of strain.
Before your therapy sessions end, your therapist will teach you ways to avoid future problems.
Sacroiliac Joint Dysfunction
A Patient’s Guide to Sacroiliac Joint Dysfunction
Introduction
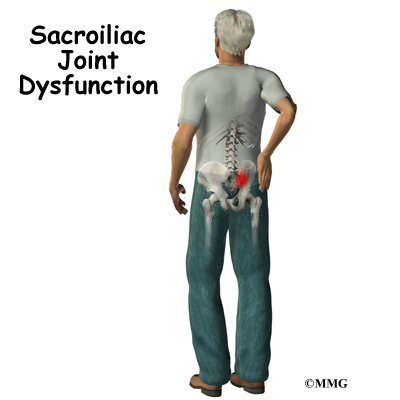
A painful sacroiliac joint is one of the more common causes of mechanical low back pain. Sacroiliac (SI) joint dysfunction is a term that is used to describe the condition – because it is still unclear why this joint becomes painful and leads to low back pain. Sacroiliac joint dysfunction can be a nuisance but it is seldom dangerous and rarely leads to the need for surgery. Most people who suffer from this problem can reduce the pain and manage the problem with simple methods.
This guide will help you understand
- how the problem develops
- how doctors diagnose the condition
- what treatment options are available
Anatomy
What part of the back is involved?
At the lower end of the spine, just below the lumbar spine lies the sacrum. The sacrum is a triangular shaped bone that is actually formed by the fusion of several vertebrae during development. The sacroiliac (SI) joint sits between the sacrum and the iliac bone (thus the name “sacroiliac” joint). You can see these joints from the outside as two small dimples on each side of the lower back at the belt line.
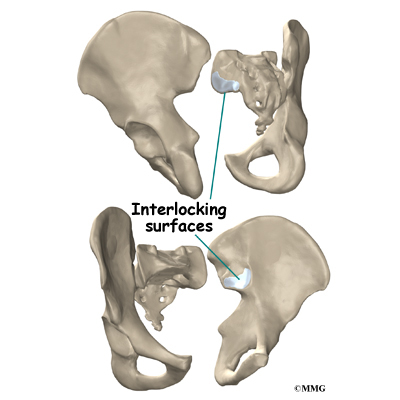
The SI joint is one of the larger joints in the body. The surface of the joint is wavy and fits together similar to the way Legos® fit together. Very little motion occurs in the SI joint. The motion that does occur is a combination of sliding, tilting and rotation. The most the joint moves in sliding is probably only a couple of millimeters, and may tilt and rotate two or three degrees.
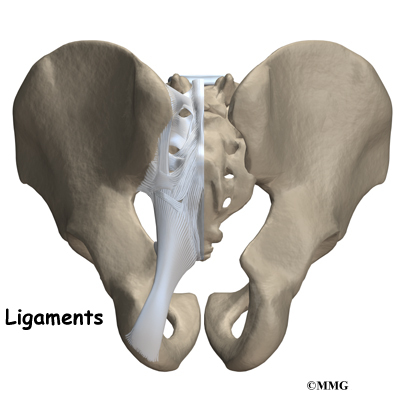
The SI joint is held together by several large, very strong ligaments. The strongest ligaments are in the back of the joint outside of the pelvis. Because the pelvis is a ring, these ligaments work somewhat like the hoops that hold a barrel together. If these ligaments are torn, the pelvis can become unstable. This sometimes happens when a fracture of the pelvis occurs and the ligaments are damaged. Generally, these ligaments are so strong that they are not completely torn with the usual injury to the SI joint.
The SI joint hardly moves in adults. During the end of pregnancy as delivery nears, the hormones that are produced causes the joint to relax. This allows the pelvis to be more flexible so that birth can occur more easily. Multiple pregnancies seem to increase the amount of arthritis that forms in the joint later in life. Other than the role the joint plays in pregnancy, it does not appear that motion is important to the function of the joint. The older one gets, the more likely that the joint is completely ankylosed, a term that means the joint has become completely stiffened with no movement at all. It appears that the primary function of the joint is to be a shock absorber and to provide just enough motion and flexibility to lessen the stress on the pelvis and spine.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Causes
What causes this problem?
There are many different causes of SI joint pain. Pregnancy may be a factor in the the development of SI joint problems later in life. Also, if a person has one leg is shorter that the other, the abnormal alignment may end up causing SI joint pain and problems. Often, an exact cause leading to a painful SI joint condition can’t be found. The joint simply gets painful, and the patient and provider don’t have an answer as to why the joint has become painful.
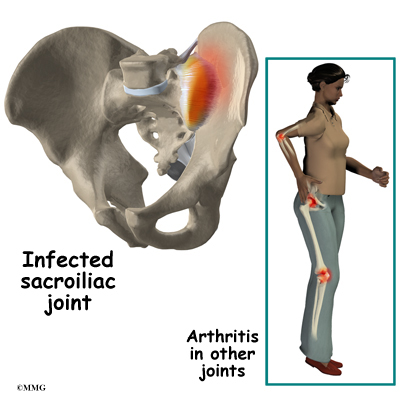
The SI joint is a synovial joint, similar to all joints such as the knee, hip and shoulder. Because of this, different types of arthritis that affect all the joints of the body will also affect the sacroiliac joint. This includes conditions such as rheumatoid arthritis, gout and psoriasis. The joint can be infected when bacteria that travel in the blood settle in the joint causing a condition called septic arthritis. This is perhaps the most worrisome cause of SI joint pain and may well require surgery to drain the infection.

Injury to the SI joint is thought to be a common cause of pain. Injury can occur during an automobile accident. One common pattern of injury occurs when the driver of a vehicle places one foot on the brake before a collision. The impact through the foot on the brake is transmitted to the pelvis causing a twisting motion to this side of the pelvis. This can injure the SI joint on that side resulting in pain. A similar mechanism occurs with a fall on one buttock. The force again causes a twisting motion to the pelvis and may injure the ligaments around the joint.
Symptoms
What does the condition feel like?
The most common symptoms from SI joint dysfunction are low back and buttock pain. The pain may affect one side or both SI joints. The pain can radiate down the leg all the way to the foot and may be confused with a herniated disc in the lumbar spine. The pain may radiate into the groin area. People often feel muscle spasm in one or both of their buttocks muscles.
Problems with the SI joint may make sitting difficult. Pain in one SI joint may cause a person to sit with that buttock tilted up. It is usually uncomfortable to sit flat in a chair.
Diagnosis
How do doctors diagnose the problem?
Diagnosis begins with a complete history and physical exam. Your doctor will ask questions about your symptoms and how the pain is affecting your daily activities. Your doctor will also want to know what positions or activities make your symptoms worse or better. You will be asked about any injuries in the past and about any other medical problems you might have such as any arthritis that runs in the family.
Your doctor then examines you by checking your posture, how you walk and where your pain is located. Your doctor checks to see which back movements cause pain or other symptoms. Your skin sensation, muscle strength, and reflexes are also tested because it is difficult to distinguish pain coming from the SI joint from pain coming from other spine conditions.
Laboratory tests may be ordered if there is any question whether you might have an infection or some type of arthritis affecting multiple joints. You may also need to have blood drawn and give a urine sample to send to the laboratory for special tests.
X-rays are commonly ordered of both the low back and pelvis. X-rays can give your doctor an idea about how much wear and tear has occurred in the SI joint. X-rays of the lumbar spine and hips are also helpful to rule out problems in these areas that may act and look like SI joint dysfunction.
Other radiological tests may be useful as well. The magnetic resonance imaging (MRI) scan can be used to look at the lumbar spine and pelvis in much more detail and to rule out other conditions in the area. The MRI scan uses magnetic waves rather than x-rays and shows a very detailed picture of the soft tissues of the body.
A computed tomography (CAT) scan may also be used to show a much more detailed look at the bone of the pelvis and the sacroiliac joint.
A bone scan is useful to see how the skeleton is reacting to any type of “stress,” such as an injury, an infection, or inflammation from arthritis. This test involves injecting chemical “tracers” into your blood stream. The tracers then show up on special spine X-rays. The tracers collect in areas where the bone tissue is reacting strongly to some type of stress to the skeleton, such as arthritis and infection of the SI joint.
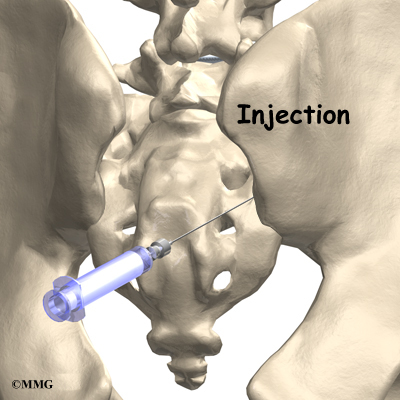
The most accurate way of determining whether the SI joint is causing pain is to perform a diagnostic injection of the joint. Because the joint is so deep, this must be done using X-ray guidance with a fluoroscope (a type of realtime X-ray). Once the doctor places a needle in the joint, an anesthetic is injected into the joint to numb the joint. If your pain goes away while the anesthetic is in the joint, then your doctor can be reasonably sure that the pain you are experiencing is coming from the SI joint.
Treatment
What treatment options are available?
Nonsurgical Treatment
Doctors often begin by prescribing nonsurgical treatment for SI joint dysfunction. In some cases, doctors simply monitor the patient’s condition to see if symptoms improve. Anti-inflammatory medications, such as ibuprofen and naproxen, are commonly used to treat the pain and inflammation in the joint. Acetominiphen (for example, Tylenol) can be used to treat the pain, but it will not control the inflammation.

Your doctor may ask that you rest your back by limiting your activities. The purpose of this is to help decrease inflammation and calm the muscle spasm. Some patients benefit from wearing a special brace called a sacroiliac belt. This belt wraps around the hips to hold the sacroiliac joint tightly together, which may ease your pain.
Patients often work with a physical therapist. After evaluating your condition, a therapist can assign positions and exercises to ease your symptoms. The therapist may design an exercise program to improve the strength and control of your back and abdominal muscles. Some therapists are trained in manipulative techniques that attempt to treat the pain in this manner. You may be able to learn how to adjust your SI joint yourself and ease the symptoms. If your physical therapist is not trained in manipulation, he/she may be able to suggest a chiropractic physician or osteopathic physician in your area who can provide this treatment.
If conservative treatment is unsuccessful, injections may be suggested by your doctor. As described above, injections are used primarily to confirm that the pain is coming from the SI joint. A series of cortisone injections may be recommended to try to reduce the inflammation in and around the SI joint. Cortisone is a powerful anti-inflammatory medication that is commonly used to control pain from arthritis and inflammation. Other medications have been injected into the joint as well. A chemical called hyaluronic acid has been used for years to treat osteoarthritis of the knee. This chemical is thought to reduce pain due to its lubricating qualities and the fact that it nourishes the articular cartilage in the synovial joints. The true mechanism of action remains unknown, but it has been used with some success in the SI joint. All of these injections are temporary and are expected to last several months at the most.
Related Document: A Patient’s Guide to Sacroiliac Joint Injections
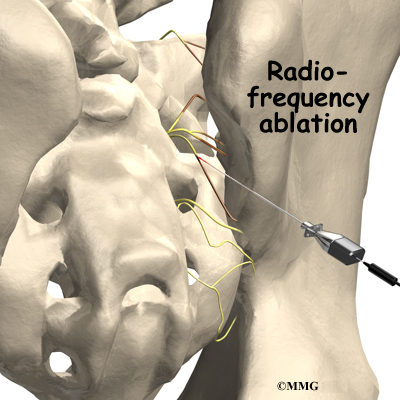
Another procedure that has been somewhat successful is called radiofrequency ablation. After a diagnostic injection has confirmed that the pain is coming from the SI joint, the small nerves that provide sensation to the joint can be “burned” with a special needle called a radiofrequency probe. In theory, this destroys any sensation coming from the joint, making the joint essentially numb. This procedure is not always successful. It is temporary but can last for up to two years. It can be repeated if needed.
Surgery
Surgery may be considered if other treatments don’t work. Surgery consists of fusing the painful SI joint. A fusion is an operation where the articular cartilage is removed from both ends of the bones forming the joint. The two bones are held together with plates and screws until the two bones grow together, or fuse, into one bone. This stops the motion between the two bones and theoretically eliminates the pain from the joint.
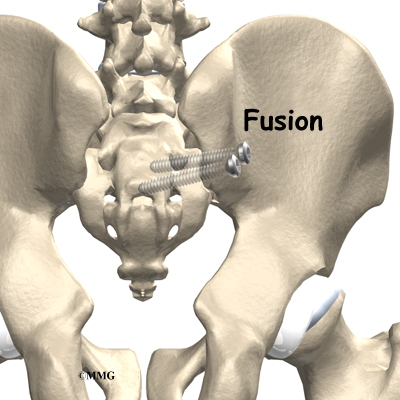
This is a big operation and is not always successful at relieving the pain. The operation is not commonly performed unless the pain is debilitating. SI joint pain is seldom this severe.
Rehabilitation
What should I expect as I recover?
Nonsurgical Rehabilitation
Doctors often recommend physical therapy for patients with SI joint dysfunction. Patients are normally seen a few times each week for four to six weeks. In severe and chronic cases, patients may need a few additional weeks of care.
When movement of a joint is limited, the pain and symptoms of SI joint dysfunction may worsen. Getting more motion can give you the relief you need for daily activities. If you don’t have full range of motion, your therapist has several ways to help you get more movement including joint manipulation, stretching, and exercises. Active movement and stretching as part of a home program can also help restore movement and get you better faster.
Therapists commonly prescribe a set of stretches to improve flexibility in the muscles of the trunk, buttocks, and thighs. In addition to the treatment you receive by your therapist, you may be given ways to help your own SI joint if your pain returns. These
exercises usually require that you position your hip and pelvis in a certain way and either stretch or contract and relax specific muscles. Follow the instructions of your therapist when doing these exercises.
If the SI joint has too much mobility and problems keep coming back, you may need extra help to stabilize the SI joint. You may be issued a SI belt to stabilize the joint. A belt like this can often ease pain enough to let you exercise comfortably.
You’ll learn some exercises to help you build strength, muscle control, and endurance in the muscles that attach around the SI joint. Unfortunately, few muscles actually connect to both the sacrum and the pelvis. Key muscles to work are the gluteus maximus, as well as the abdominal and low back muscles.
After Surgery
You will normally need to wait at least six weeks before beginning a rehabilitation program after having SI joint fusion surgery. You should plan on attending therapy sessions for six to eight weeks. Expect full recovery to take up to six months.
During therapy after SI joint surgery, your therapist may use treatments such as heat or ice, electrical stimulation, massage, and ultrasound to help calm your pain and muscle spasm. Then you’ll begin learning how to move safely with the least strain on the healing area.
As your rehabilitation program evolves, you’ll begin doing more challenging exercises. The goal is to safely advance your strength and function.
As your therapy sessions come to an end, your therapist helps you get back to the activities you enjoy. Ideally, you’ll be able to resume your normal activities. You may need guidance on which activities are safe or how to change the way you go about your
activities.
When treatment is well under way, regular visits to your therapist’s office will end. Your therapist will continue to be a resource. But you’ll be in charge of doing your exercises as part of an ongoing home program.
Piriformis Syndrome
A Patient’s Guide to Piriformis Syndrome
Introduction
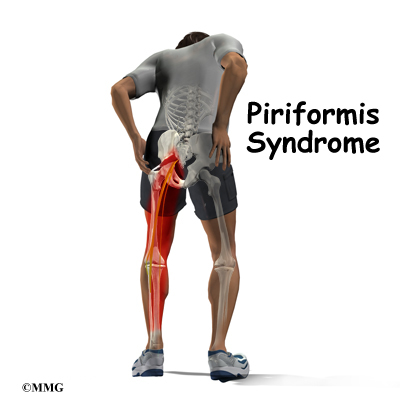
Pain in the buttock that radiates down the leg is commonly called sciatica. The most common cause for sciatica is irritation of the spinal nerves in or near the lumbar spine. Sometimes the nerve irritation is not in the spine but further down the leg. One possible cause of sciatica is piriformis syndrome. Piriformis syndrome can be painful, but it is seldom dangerous and rarely leads to the need for surgery. Most people with this condition can reduce the pain and manage the problem with simple methods, such as physical therapy.
This guide will help you understand
- how the problem develops
- how doctors diagnose the condition
- what treatment options are available
Anatomy
What parts of the body are involved?
The lower lumbar spinal nerves leave the spine and join to form the sciatic nerve. The sciatic nerve leaves the pelvis through an opening called the sciatic notch.
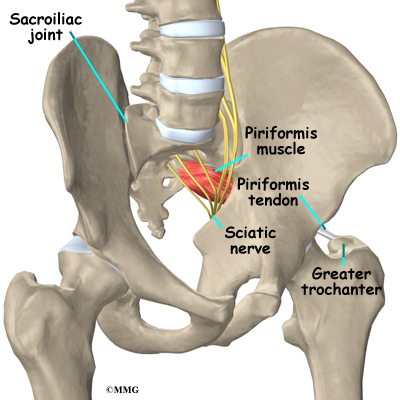
The piriformis muscle begins inside the pelvis. It connects to the sacrum, the triangular shaped bone that sits between the pelvic bones at the base of the spine. The connection of the sacrum to the pelvis bones forms the sacroiliac joint. There is one sacroiliac joint on the left and one on the right of the low back. The other end of the piriformis muscle connects by a tendon to the greater trochanter, the bump of bone on the top side of your hip.
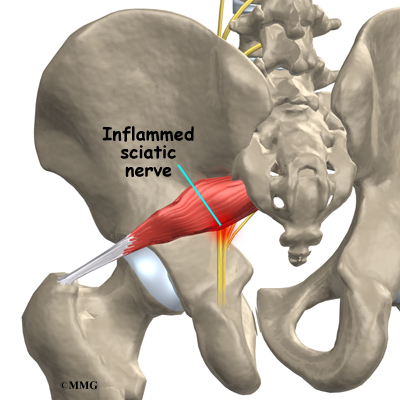
The piriformis muscle is one of the external rotators of the hip and leg. This means that as the muscle works, it helps to turn the foot and leg outward. Problems in the piriformis muscle can cause problems with the sciatic nerve. This is because the sciatic nerve runs under (and sometimes through) the piriformis muscle on its way out of the pelvis. The piriformis muscle can squeeze and irritate the sciatic nerve in this area, leading to the symptoms of sciatica.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Causes
What causes this problem?
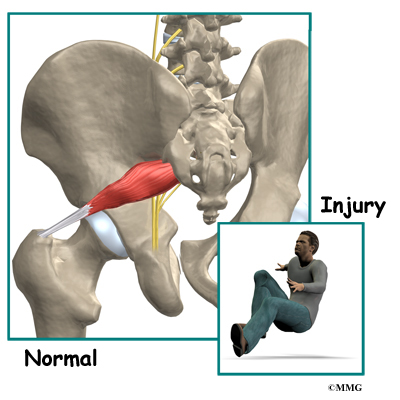
The symptoms of sciatica come from irritation of the sciatic nerve. It’s still a mystery why the piriformis muscle sometimes starts to irritate the sciatic nerve. Many doctors think that the condition begins when the piriformis muscle goes into spasm and tightens
against the sciatic nerve, squeezing the nerve against the bone of the pelvis.
In some cases, the muscle may be injured due to a fall onto the buttock. Bleeding in and around the piriformis muscle forms a hematoma. A hematoma describes the blood that has pooled in that area.
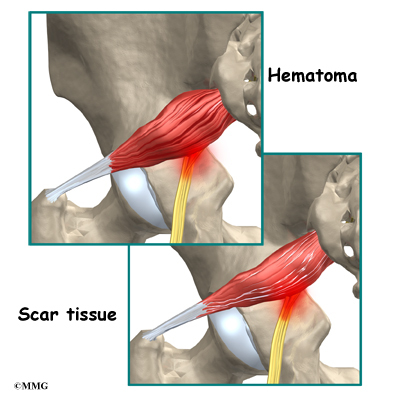
The piriformis muscle begins to swell and put pressure on the sciatic nerve. Soon the hematoma dissolves, but the muscle goes into spasm.
The sciatic nerve stays irritated and continues to be a problem. Eventually the muscle heals, but some of the muscle fibers inside the piriformis muscle are replaced by scar tissue. Scar tissue is not nearly as flexible and elastic as normal muscle tissue. The
piriformis muscle can tighten up and put constant pressure against the sciatic nerve.
Symptoms
What does the condition feel like?
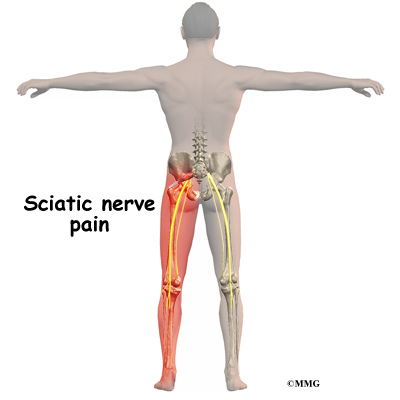
Piriformis syndrome commonly causes pain that radiates down the back of the leg. The pain may be felt only on one side, though it is sometimes felt on both sides. The pain can radiate down the leg all the way to the foot and may be confused for a herniated disc in the lumbar spine. Changes in sensation and weakness in the leg or foot are rare. Some people say they feel a sensation of vague tingling down the leg.
Sitting may be difficult. Usually people with piriformis syndrome do not like to sit. When they do sit down, they tend to sit with the sore side buttock tilted up rather than sitting flat in the chair.
Diagnosis
How do doctors diagnose the problem?
Diagnosis begins with a complete history and physical exam. Your doctor will ask questions about your symptoms and how the pain is affecting your daily activities. Your doctor will also want to know what positions or activities make your symptoms worse or better. You will be asked about any injuries in the past and about any other medical problems you might have such as any arthritis that runs in the family.
Next the doctor examines you by checking your posture, how you walk, and where your pain is located. Your doctor checks to see which back movements cause pain or other symptoms.
Your skin sensation, muscle strength, and reflexes are also tested because it is difficult to distinguish pain coming from the sacroiliac joint from pain coming from other spine conditions.
If there is any question whether you might have an infection or some type of arthritis affecting multiple joints, laboratory tests may be ordered. You may need to have blood drawn and give a urine sample to send to the laboratory for special tests.
X-rays are commonly ordered of both the low back and pelvis. X-rays can give your doctor an idea about how much wear and tear has developed in the sacroiliac joint. X- rays of the lumbar spine and hips are also helpful to rule out problems in these areas that may look and act like sacroiliac joint problems.
Other radiological tests may also be useful. A magnetic resonance imaging (MRI) scan can be used to look at the lumbar spine and pelvis in much more detail and rule out other conditions in the area conditions. The MRI scan uses magnetic waves rather than X-rays and shows a very detailed picture of the soft tissues of the body.
A special type of MRI scan called neurography is being used more frequently to look at nerves. This uses a regular MRI scanner, but the computer settings are set to look for areas of irritation along a nerve. This may change the way doctors use the MRI to diagnose nerve problems such as piriformis syndrome, thoracic outlet syndrome, and carpal tunnel syndrome.
A bone scan is useful to see how the skeleton is reacting to any type of “stress,” such as an injury, an infection, or inflammation from arthritis. Chemical “tracers” are injected into your blood stream. The tracers then show up on special spine X- rays. The tracers collect in areas where the bone tissue is reacting strongly to some type of stress to the skeleton, such as arthritis and infection of the sacroiliac joint.
The most accurate way to tell if the piriformis muscle is the cause of pain is with a diagnostic injection into the muscle. The muscle is deep inside the buttock, so the injection requires X-ray guidance with a fluoroscope, a CT scanner, or an open MRI machine. Once the needle is placed in the muscle, an anesthetic can be injected into the muscle to paralyze the piriformis muscle. If the pain goes away after the injection, your doctor can be reasonably sure that the pain you are feel is from piriformis syndrome.
Treatment
What treatment options are available?
Nonsurgical Treatment
Doctors often begin by prescribing nonsurgical treatment for piriformis syndrome. In some cases, doctors simply monitor their patients’ condition to see if symptoms improve. Anti-inflammatory medications, such as ibuprofen and naproxen, are commonly used to treat the pain and inflammation caused by the irritation on the nerve. Acetaminophen (for example Tylenol®) can be used to treat the pain but will not control the inflammation.
You’ll probably work with a physical therapist. After evaluating your condition, the therapist uses treatments to ease spasm and pain in the piriformis muscle. Exercises, particularly stretching exercises, are given to try and relieve irritation on the sciatic nerve.

If you still have pain after trying these treatments, your doctor may suggest injections.The main use of injections is to see if your pain is from piriformis syndrome. An injection of local anesthetic such as lidocaine can be injected into the muscle to temporarily relax it. This loosens up the muscle and reduces the irritation on the sciatic nerve. Other medications have also been injected into the piriformis muscle. Cortisone, for example, may be mixed with the anesthetic medication to reduce the inflammation on the sciatic nerve. Cortisone is a potent anti-inflammatory medication that is commonly used both in pill form and in injections to treat inflammation.
Related Document: A Patient’s Guide to Piriformis Muscle Injections
Botulism injection therapy (also known as Botox® injections) can be used to actually paralyze the piriformis muscle. This makes the muscle relax, which helps take pressure off the sciatic nerve. The effect of the Botox® injection isn’t permanent; it generally only lasts a few months. In the meantime, however, it is hoped that a stretching program can be used to fix the problem. In other words, when the injection wears off, the muscle may have been stretched enough so that the symptoms do not return.
Surgery
Surgery may be considered but usually only as a last resort. There are two procedures in use. The first is to cut the piriformis tendon where it attaches on the greater trochanter (the bump on the side of your hip). The other method is to cut through the piriformis muscle to take pressure off the sciatic nerve.
These procedures are usually done on an outpatient basis, meaning that you will be able to go home the same day as the surgery. In some cases, you may need to stay in the hospital for one night. Both procedures can be done under general anesthesia or under a spinal type of anesthetic.
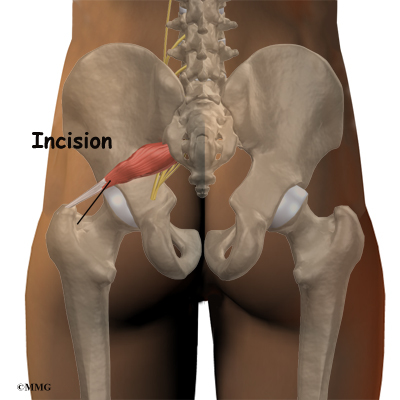
The surgeon begins by making a small incision, usually about three inches long, in the buttock. The fibers of the gluteus maximus, the largest buttock muscle, are split. This gives the surgeon a way to see deep into the buttock and locate the piriformis muscle. When the piriformis muscle and tendon can be seen, the surgeon then cuts (releases) the tendon where it connects to the greater trochanter.
If more room is needed to release the pressure on the nerve, a portion of the piriformis muscle may be removed.
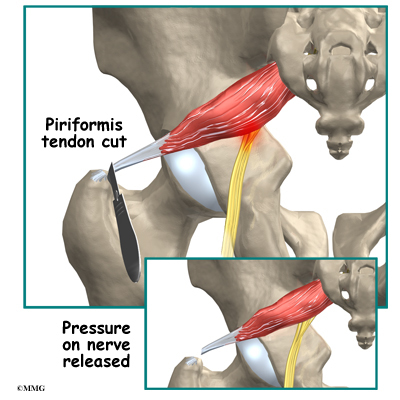
This usually doesn’t cause problems with strength because there are several much stronger muscles that help turn the leg outward.
Rehabilitation
What should I expect as I recover?
Nonsurgical Rehabilitation
Most patients with piriformis syndrome work with a physical therapist. Plan to attend physical therapy sessions two to three times each week for six to eight weeks.
Your therapist begins by evaluating your condition. This includes attention to the low back, as well as the sacroiliac and hip joints.
Physical therapy treatments for piriformis syndrome often begin with heat applications. Heat is used to help the piriformis muscle relax, easing spasm and pain. Your physical therapist may place a hot pack over your buttocks muscle.
Ultrasound is another treatment choice that can be set for deep heating in the buttock area. Ultrasound uses high frequency sound waves that are directed through the skin. The deep heating effect of ultrasound is ideal for preparing the piriformis muscle for hands-
on forms of treatment and for getting the muscle to stretch out.
Hands-on treatments such as deep massage and specialized forms of soft-tissue mobilization may be used initially. Your therapist may also position your hip and leg in a way that helps to relax nerve signals to the piriformis.
The keystone treatment for piriformis treatment is stretching. Stretching is especially effective following heat and hands on treatments. Your therapist will position you in ways that help you get a good stretch on the piriformis muscle. Along with the stretches
you’ll do in the clinic, you’ll be shown several ways to stretch the muscle on your own. You need to do your stretches every few hours. Be gentle and cautious as you stretch to avoid overdoing it.
As your symptoms ease, your therapist will gradually advance your program to include posture training, muscle strengthening, and general conditioning.
After Surgery
Your surgeon may prescribe physical therapy after surgery for piriformis syndrome. You’ll probably only need to attend sessions for four to six weeks. Expect full recovery to take up to three months.
During therapy after surgery, your therapist may use treatments such as heat or ice, electrical stimulation, massage, and ultrasound to help calm pain and muscle spasm. Then you’ll begin learning how to move safely with the least strain on the healing area.
As the rehabilitation program evolves, you’ll begin doing more challenging exercises. The goal is to safely advance strength and function.
As the therapy sessions come to an end, your therapist helps you get back to the activities you enjoy. Ideally, you’ll be able to resume normal activities. You may need guidance on which activities are safe or how to change the way they go about their activities.
When treatment is well under way, regular visits to your therapist’s office will end. Your therapist will continue to be a resource. But you’ll be in charge of doing your exercises as part of an ongoing home program.
Back Care Boot Camp
![]()
No treatment program for low back pain is complete without a great deal of attention to the prevention of further back problems.
It is a common belief that most episodes of low back pain simply get better in 6 or 8 weeks no matter what type of treatment a patient receives. The problem with this thinking is that 90 percent of these patients will have recurring bouts of back pain. Without proper instruction on how to protect the spine, they will continue to do things that lead to further injury and deterioration of the spine. Without information about how to practice good spine health, patients are at risk for having increasing problems with low back pain and are more apt to eventually develop disabling back pain.
The truth is that most people who’ve had back pain once don’t get completely better by themselves. They may begin to have less pain, but that isn’t always a sign that everything has returned to normal.

Scientists have determined that having back pain, even once, can alter the way your back and abdominal muscles work, which can leave your spine unsupported and prone to another injury. That’s where Back Care Boot Camp comes in. It details these new facts. It also teaches you ways to energize your muscles again to protect your back and to reduce the chances of having a future problem. Back Care Boot Camp gives immediate guidance to help you head off potential long-term problems—before they occur.
The Back Care Boot Camp program is designed to be used with a physical therapist as a guide. The program consists of 8 formal sessions of physical therapy and usually takes about four weeks to complete. The progam is designed to educate you about the importance of spine health and give you the proper tools to protect your spine into the future.
The entire program is available online at:
or you can purchase a printed manual in a high quality,
full color softback book format here:
Lumbar Spondylolysis
A Patient’s Guide to Lumbar Spondylolysis
Introduction
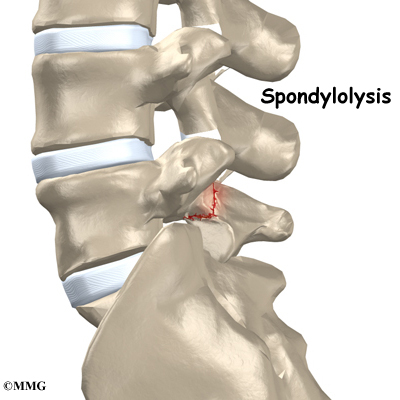
Spondylolysis happens when a crack forms in the bony ring on the back of the spinal column. Most commonly, this occurs in the low back. In this condition, the bone that protects the spinal cord fractures as a result of excessive or repeated strain. The area affected is called the pars interarticularis, so doctors sometimes refer to this condition as a pars defect.
This condition appears in six percent of children. It mainly affects young athletes who participate in sports in which the spine is repeatedly bent backwards, such as gymnastics, football, and karate.
Although spondylolysis can affect people of any age, children and adolescents are most susceptible. This is because their spines are still developing, and the pars is the weakest part of the vertebra. Placing extra strain on this area of the spine during childhood increases the chance that a pars defect will occur.
This guide will help you understand
- how the problem develops
- how doctors diagnose the condition
- what treatment options are available
Anatomy
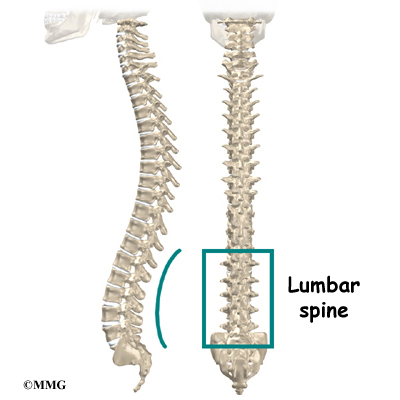
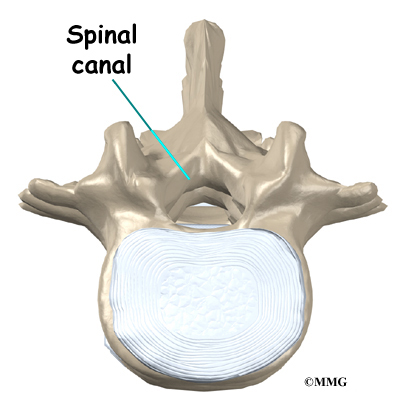
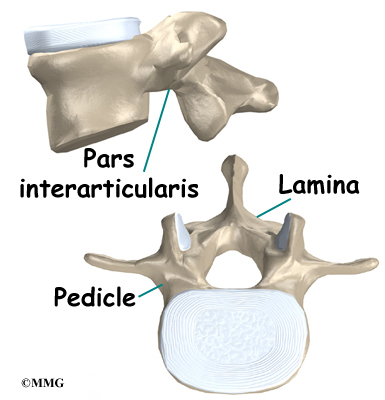
What parts of the spine are involved?
The human spine is made up of 24 spinal bones, called vertebrae. Vertebrae are stacked on top of one another to create the spinal column. The spinal column gives the body its form. It is the body’s main upright support. The section of spine in the lower back is called the lumbar spine.
Each vertebra is formed by a round block of bone, called a vertebral body. A circle of bone attaches to the back of the vertebra. When the vertebrae are stacked on top of each other, these bony rings create a hollow tube. This tube, called the spinal canal, surrounds the spinal cord as it passes through the spine. Just as the skull protects the brain, the bones of the spinal column protect the spinal cord.
The protective ring that surrounds the spinal cord is a continuous ring of bone. Its sections include two pedicles which attach directly to the back of the vertebral body. Two laminae complete the ring.
The pedicles and laminae are two different areas of the bony ring. The area between them is not a joint. Rather, it is a location in the continuous ring of bone that doctors call the pars interarticularis, or “pars” for short. There are two such meeting points on the back of each vertebra, one on the left and one on the right. The pars is thought to be the weakest part of the bony ring.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Causes
What causes this problem?
Spondylolysis is thought to be caused by repeated strains that damage the lower spine over time. The repeated strains can eventually lead to an overuse injury in the pars interarticularis. The most common location for this to occur is in the lowest vertebra of the spine, which doctors call L5. This vertebra connects the spine to the pelvis. However, a problem with the pars can occur in any lumbar vertebra. It rarely happens in more than one vertebra at a time.

The vertebra initially responds to the abnormal strain by adding new bone cells around the injured area. But if the injuries happen faster than the body can keep up with needed repairs, a crack may form in the weakened bone. This is called a stress fracture. This type of fracture occurs in the pars, the area of bony ring between the pedicle and lamina.
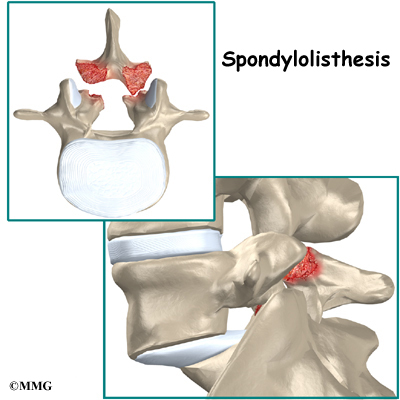
The crack may affect only one side of the bony ring. However, it is equally common for the defect to occur on both sides. When this happens, the vertebra is no longer held firmly in place by the facet joints on the back of the ring. As a result, the vertebra is free to slip forward over the one below. This slippage, which is closely related to spondylolysis, is called spondylolisthesis.
Related Document: A Patient’s Guide to Spondylolisthesis

Spondylolysis commonly occurs in young gymnasts who regularly practice backbends as part of their routines. Football linemen and dancers are also prone to spondylolysis. Symptoms sometimes appear when an athlete quickly ramps up his or her training intensity, applies incorrect technique, or uses poor equipment.
Symptoms
What does the condition feel like?
People with spondylolysis may feel pain and stiffness in the center of the low back. Bending fully backward increases pain. Symptoms typically get worse with activity and go away with rest. Doctors refer to this type of back pain as mechanical pain because it most likely comes from excess movement between the vertebrae.
Individuals may eventually experience pain that radiates down one or both legs. This pain may come from pressure and irritation on the nerves that exit the spinal canal near the fracture. When nerve pressure in the low back causes leg pain, doctors refer it as neurogenic pain.

The cause of this nerve pressure is a result of the body’s attempt to heal the stress fracture. Over time, the healing process may cause a bump of extra cartilage to grow at the site where the bones are trying to heal the overuse injury. If too much cartilage builds up, this bump may intrude into the opening where the nerves exit the spine. The bump may squeeze the nerve. This can produce pain and weakness in the leg. Reflexes become slowed. The person may also notice a pins and needles sensation in the skin where the spinal nerve travels.
Diagnosis
How do doctors diagnose the problem?
Diagnosis begins with a complete history and physical exam. Your doctor will ask questions about your symptoms and how the problem is affecting your daily activities. You will be asked about your involvement in sports and your level of performance. Doctors may suspect a problem with spondylolysis in football linemen, gymnasts, and those in similar sports that require intensive levels of performance. Your doctor will also want to know what positions or activities make your symptoms worse or better.
Next the doctor examines you by checking your posture and the amount of movement in your low back. Your doctor checks to see which back movements cause pain or other symptoms. Your skin sensation, muscle strength, and reflexes are also tested.
Your doctor may order an X-ray of your low back. An angled, or oblique, view is often used to check for a pars fracture. The doctor traces around the vertebral body and bony ring on the X-ray film. The outline normally forms an image that looks like a small dog. When a crack is present, however, the dog will appear to have a collar around its neck. This is referred to as the Scotty dog sign. It confirms a diagnosis of spondylolysis.
Small defects in the bone may not show up on X-ray. Also, a recent stress fracture won’t always appear on X-ray. As a result, your doctor may order a bone scan to get the most accurate information. This involves injecting chemical “tracers” into your blood stream. The tracers then show up on special spine X-rays. The tracers collect in areas of extra stress to bone tissue, such as a stress fracture of the pars interarticularis.
Computed tomography (a CT scan) may be ordered. This is a detailed X-ray that lets doctors see slices of the body’s tissue. The image can show if the edges of the fractured bone have begun growing together. The scan shows whether the fracture is new or old, so doctors can decide which treatments will help the most.
When more information is needed, your doctor may order a magnetic resonance imaging (MRI) scan. The MRI machine uses magnetic waves rather than X-rays to show the soft tissues of the body. It can help in the diagnosis of spondylolysis. It can also provide information about the health of nearby intervertebral discs and other soft tissues that don’t appear on X-rays.
Treatment
What treatment options are available?
Nonsurgical Treatment
Doctors often begin by prescribing nonsurgical treatment for spondylolysis. This is because symptoms from these stress fractures often resolve with rest or bracing. In some cases, doctors simply monitor their patients’ condition to see if symptoms improve. An X-ray may be taken every few months to check how well the area is healing.
If the doctor feels that the problem is due to a recent fracture, you may be placed in a rigid back brace or cast for three to four months. Keeping the spine from moving can help ease pain and inflammation. It can also improve the chances the bones will grow back together. Most people who require a brace or cast overcome symptoms and are able to eventually get back to activities free of pain. This can happen even when follow-up tests show that the bones haven’t completely healed.
Your doctor may ask that you rest your back by limiting your activities. The purpose of this is to help decrease inflammation and calm muscle spasm. You may need to take some time away from your sport, especially if it requires repeated back bending. This gives your back a chance to heal. Most patients who follow these measures get better. Patients are rarely counseled to completely discontinue participating in their sport, and only in severe cases.
Patients often work with a physical therapist. After evaluating your condition, a therapist can assign positions and exercises to ease your symptoms. The therapist may design an exercise program to improve the strength and control of your back and abdominal muscles. By watching you perform your sport activity, your therapist can suggest style, technique, or equipment changes to improve your performance and prevent future problems.
Surgery
Most patients with spondylolysis do not require surgery. When symptoms are not relieved with nonsurgical treatments, however, patients may require surgery. The main types of surgery for spondylolysis include
- laminectomy
- posterior lumbar fusion
Laminectomy

Nerve compression can cause considerable pain and symptoms. If too much cartilage builds up where the fractured bones are trying to heal, the nerve that passes near the injured bone may get squeezed, as described earlier. To fix this, a section of the bony ring is removed to take pressure off the nerve. The procedure to remove the lamina from the bony ring and release pressure on the nerve is called laminectomy.
Related Document: A Patient’s Guide to Lumbar Laminectomy
Posterior Lumbar Fusion
A spinal fusion may be required after a surgeon performs a laminectomy procedure. Fusion is recommended when a spinal segment (a set of vertebrae) has become too loose or unstable.
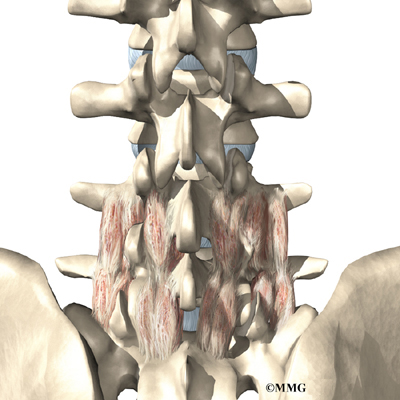
A spinal fusion allows two or more bones to grow together, or fuse, into one solid bone. This keeps the bones and joints from moving. In this procedure, the surgeon lays small grafts of bone over the problem area on the back of the spine. Some surgeons also apply metal plates and screws to prevent the two vertebrae from moving. However, this practice is controversial because fusion occurs in about 90 percent of children with spondylolysis when the procedure is done without plates and screws.
Related Document: A Patient’s Guide to Posterior Lumbar Fusion
Rehabilitation
What should I expect as I recover?
Nonsurgical Rehabilitation
Recovery from this condition is much like nonsurgical treatment mentioned earlier. Once you have rested your back to allow it to heal, your doctor may recommend that you work with a physical therapist a few times each week for four to six weeks. In severe cases, patients may need a few additional weeks of physical therapy.
The first goal of treatment is to control symptoms. The therapist works with you to find positions and movements that ease pain. Treatments of heat, cold, ultrasound, and electrical stimulation may be used to calm pain and muscle spasm.
As you recover, you will gradually advance in a series of strengthening exercises for the abdominal and low back muscles. Working these core muscles helps patients begin moving easier and lessens the chances of future pain and problems.
When needed, a therapist can work closely with a sports coach on strategies for a patient’s safe return to his or her sport. The two may provide suggestions on technique, equipment, and training frequency and intensity.

If the patient is a working adult, the therapist may also work with the patient’s doctor and employer to help the patient get back on the job as quickly as reasonably possible. The patient may be required to do lighter duties at first. As soon as the patient is able, he or she will do normal work activities. The therapist may also suggest changes that could help the patient work safely, with less chance of re-injuring his or her back.
A primary purpose of therapy is to help patients learn how to take care of their symptoms and prevent future problems. Patients are given a home program of exercises to continue improving flexibility, posture, endurance, and low back and abdominal strength. The therapist also describes strategies you can use if your symptoms flare up.
Most adolescents get better after wearing a brace or cast for three months. Even then, a CT scan sometimes shows an unhealed fracture. In these cases, however, symptoms often go away completely, allowing a safe return to sports. Patients do best when guided in a gradual manner with the supervision of a therapist and sports coach.
After Surgery
Rehabilitation after surgery is more complex. Some patients leave the hospital shortly after surgery. However, some surgeries require patients to stay in the hospital for a few days. Patients who stay in the hospital may visit with a physical therapist in the hospital room soon after surgery. The treatment sessions help patients learn to move and do routine activities without putting extra strain on the back.
During recovery from surgery, patients should follow their surgeon’s instructions about wearing a back brace or support belt. They should be cautious about overdoing activities in the first few weeks after surgery.
Many surgical patients need physical therapy outside of the hospital. Patients who’ve had lumbar fusion surgery normally need to wait at least six weeks before beginning a rehabilitation program. This delay gives the fusion a chance to start healing. Patients typically need to attend therapy sessions for six to eight weeks and should expect full recovery to take up to six months.
Lumbar Spondylolisthesis
A Patient’s Guide to Lumbar Spondylolisthesis
Introduction
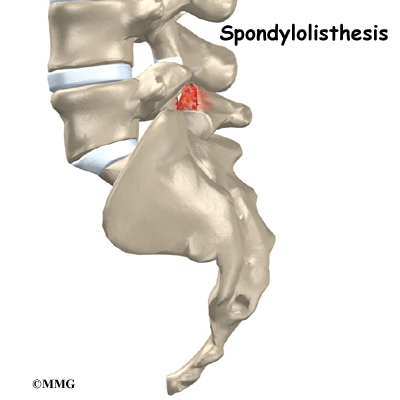
Normally, the bones of the spine (the vertebrae) stand neatly stacked on top of one another. Ligaments and joints support the spine. Spondylolisthesis alters the alignment of the spine. In this condition, one of the spine bones slips forward over the one below it. As the bone slips forward, the nearby tissues and nerves may become irritated and painful.
This guide will help you understand
- how the problem develops
- how doctors diagnose the condition
- what treatment options are available
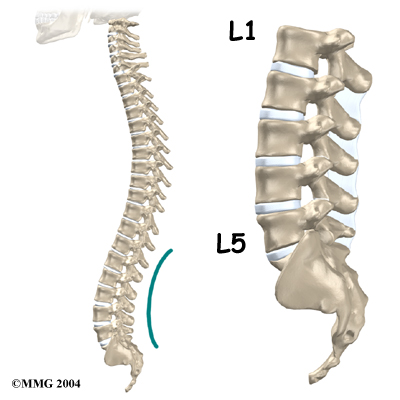
Anatomy
What parts of the spine are involved?
The human spine is made up of 24 spinal bones, called vertebrae. Vertebrae are stacked on top of one another to create the spinal column. The spinal column gives the body its form. It is the body’s main upright support. The section of the spine in the lower back is called the lumbar spine.
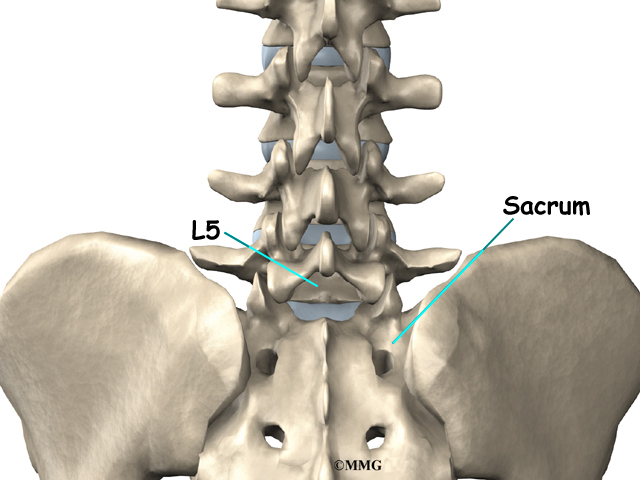
The lumbar spine is made of the lower five vertebrae. Doctors often refer to these vertebrae as L1 to L5. These five vertebrae line up to give the low back a slight inward curve. The lowest vertebra of the lumbar spine, L5, connects to the top of the sacrum, a triangular bone at the base of the spine that fits between the two pelvic bones.
Each vertebra is formed by a round block of bone, called a vertebral body.
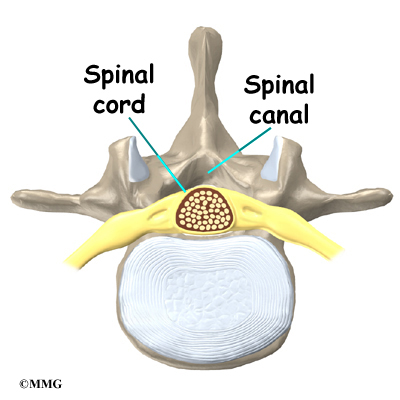
A circle of bone attaches to the back of the vertebral body. When the vertebrae are stacked on top of each other, these bony rings create a hollow tube. This tube, called the spinal canal, surrounds the spinal cord as it passes through the spine. Just as the skull protects the brain, the bones of the spinal column protect the spinal cord.

The spinal cord only extends to L2. Below this level, the spinal canal encloses a bundle of nerves that goes to the lower limbs and pelvic organs. The Latin term for this bundle of nerves is cauda equina, meaning horse’s tail.
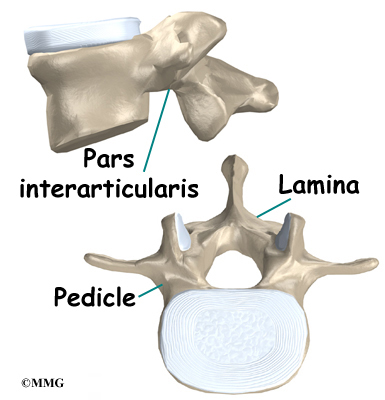
Two sets of bones form the spinal canal’s bony ring. Two pedicle bones attach to the back of each vertebral body. Two lamina bones complete the ring. The place where the lamina and pedicle bones meet is called the pars interarticularis, or pars for short. There are two such meeting points on the back of each vertebra, one on the left and one on the right. The pars is thought to be the weakest part of the bony ring.
Intervertebral discs separate the vertebral bodies. The discs normally work like shock absorbers. They protect the spine against the daily pull of gravity. They also protect the spine during strenuous activities that put strong force on the spine, such as jumping, running, and lifting.

The lumbar spine is supported by ligaments and muscles. The ligaments, which connect bones together, are arranged in layers and run in multiple directions. Thick ligaments connect the bones of the lumbar spine to the sacrum (the bone below L5) and pelvis.
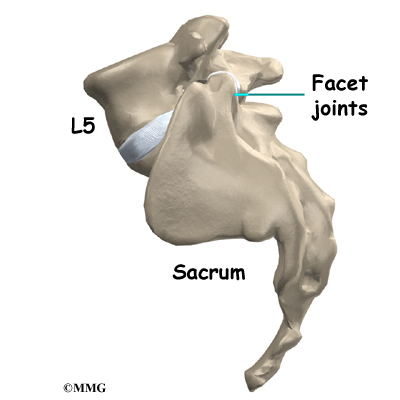
Between the vertebrae of each spinal segment are two facet joints. The facet joints are located on the back of the spinal column. There are two facet joints between each pair of vertebrae, one on each side of the spine. A facet joint is made of small, bony knobs that line up along the back of the spine. Where these knobs meet, they form a joint that connects the two vertebrae. The alignment of the facet joints of the lumbar spine allows freedom of movement as you bend forward and back.
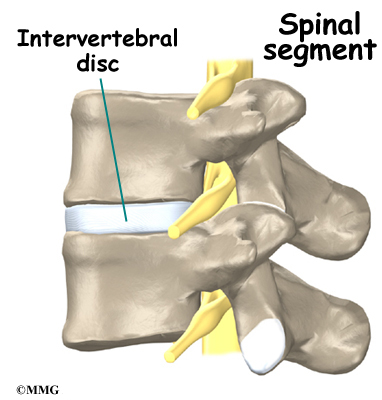
The anatomy of the lumbar spine is often discussed in terms of spinal segments. Each spinal segment includes two vertebrae separated by an intervertebral disc, the nerves that leave the spinal cord at that level, and the facet joints that link each level of the spinal column.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Causes
Why do I have this problem?
Spondylolisthesis may very rarely be congenital, which means it is present at birth. It can also occur in childhood as a result of injury. In older adults, degeneration of the disc and facet (spinal) joints can lead to spondylolisthesis.
Spondylolisthesis from degeneration usually affects people over 50 years old. This condition occurs in African Americans more often than in whites. Women are affected more often than men. The effect of the female hormone estrogen on ligaments and joints is to cause laxity or looseness. The higher levels of estrogen in women may account for the greater incidence of spondylolisthesis. Degenerative spondylolisthesis mainly involves slippage of L4 over L5.
In younger patients (under 20 years old), spondylolisthesis usually involves slippage of the fifth lumbar vertebra over the top of the sacrum. There are several reasons for this. First, the connection of L5 and the sacrum forms an angle that is tilted slightly forward, mainly because the top of the sacrum slopes forward. Second, the slight inward curve of the lumbar spine creates an additional forward tilt where L5 meets the sacrum. Finally, gravity attempts to pull L5 in a forward direction.
Facet joints are small joints that connect the back of the spine together. Normally, the facet joints connecting L5 to the sacrum create a solid buttress to prevent L5 from slipping over the top of the sacrum. However, when problems exist in the disc, facet joints, or bony ring of L5, the buttress becomes ineffective. As a result, the L5 vertebra can slip forward over the top of the sacrum.
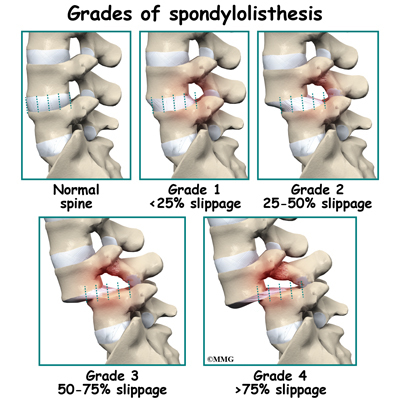
A condition called spondylolysis can lead to the slippage that happens with spondylolisthesis. Spondylolysis is a defect in the bony ring of the spinal column. It affects the pars interarticularis, mentioned earlier. This defect is most commonly thought to be a stress fracture that happens from repeated strains on the bony ring. Participants in gymnastics and football commonly suffer these strains. Spondylolysis can lead to the spine slippage when a fracture occurs on both sides of the bony ring. This slippage is called spondylolisthesis. The slippage is graded from I through IV, one being mild, IV often causing neurological symptoms. The back section of the bony ring separates from the main vertebral body, so the injured vertebra is no longer connected by bone to the one below it. In this situation, the facet joints can’t provide their normal support. The vertebra on top is then free to slip forward over the one below.
View animation of spondylolisthesis
Related Document: A Patient’s Guide to Spondylolysis
A traumatic fracture in the bony ring can lead to slippage when the fracture goes completely through both sides of the bony ring. The facet joints are no longer able to provide a buttress, allowing the vertebra with the crack in it to slip forward. This is similar to what happens when spondylolysis (mentioned earlier) occurs on both sides of the bony ring, but in this case it happens all at once.
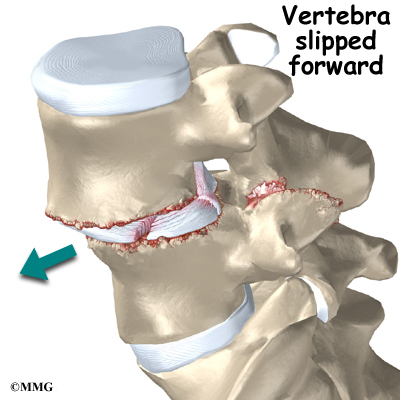
Degenerative changes in the spine (those from wear and tear) can also lead to spondylolisthesis. The spine ages and wears over time, much like hair turns gray. These changes affect the structures that normally support healthy spine alignment. Degeneration in the disc and facet joints of a spinal segment causes the vertebrae to move more than they should. The segment becomes loose, and the added movement takes an additional toll on the structures of the spine. The disc weakens, pressing the facet joints together. Eventually, the support from the facet joints becomes ineffective, and the top vertebra slides forward.
Symptoms
What does the condition feel like?
An ache in the low back and buttock areas is the most common complaint in patients with spondylolisthesis. Pain is usually worse when standing, walking, or bending backward and may be eased by resting or bending the spine forward. Leaning on a counter top, piece of furniture, or shopping cart are common ways to alleviate (reduce) the symptoms.
Spasm is also common in the low back muscles. The hamstring muscles on the back of the thighs may become tight.
The pain can be from mechanical causes. Mechanical pain is caused by wear and tear on the parts of the spine. When the vertebra slips forward, it puts a painful strain on the disc and facet joints.
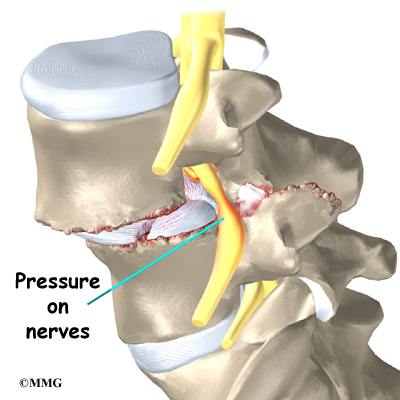
Slippage can also cause nerve compression. Nerve compression is a result of pressure on a nerve. As the spine slips forward, the nerves may be squeezed where they exit the spine. This condition also reduces space in the spinal canal where the vertebra has slipped. This can put extra pressure on the nerve tissues inside the canal. Nerve compression can cause symptoms where the nerve travels and may include numbness, tingling, slowed reflexes, and muscle weakness in the legs.
Nerve pressure on the cauda equina (mentioned earlier), the bundle of nerve roots within the lumbar spinal canal, can affect the nerves that go to the bladder and rectum. When this happens, bowel and/or bladder function can be affected. The pressure may cause low back pain, pain running down the back of both legs, and numbness or tingling between the legs in the area you would contact if you were seated on a saddle.
Diagnosis
How do doctors diagnose the problem?
Diagnosis begins with a complete history and physical exam. Your doctor will ask questions about your symptoms and how your problem is affecting your daily activities. Your doctor will also want to know what positions or activities make your symptoms worse or better.
Next the doctor examines you by checking your posture and the amount of movement in your low back. Your doctor checks to see which back movements cause pain or other symptoms. Your skin sensation, muscle strength, and reflexes are also tested.
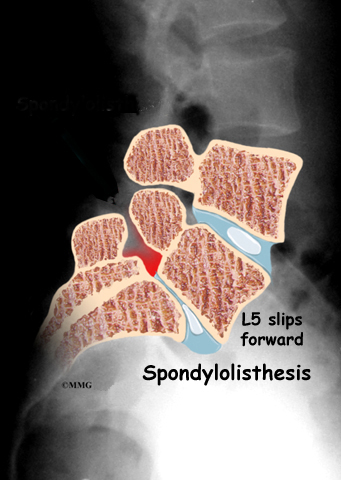
Doctors will usually order X-rays of the low back. The X-rays are taken with your spine in various positions. They can be used to see which vertebra is slipping and how far it has slipped.
If more information is needed, your doctor may order computed tomography (a CT scan). This is a detailed X-ray that lets the doctor see slices of the body’s tissue. If you have nerve problems, the doctor may combine the CT scan with myelography. To do this, a special dye is injected into the space around the spinal canal, the subarachnoid space. During the CT scan, the dye highlights the spinal nerves. The dye can improve the accuracy of a standard CT scan for diagnosing the health of the nerves.
Your doctor may also order a magnetic resonance imaging (MRI) scan. The MRI machine uses magnetic waves rather than X-rays to show the soft tissues of the body. It can help in the diagnosis of spondylolisthesis. It can also provide information about the health of nerves and other soft tissues.
Treatment
What treatment options are available?
Nonsurgical Treatment
Studies have not been done yet to determine the best treatment for this condition. Conservative care is preferred, especially when the vertebra hasn’t slipped very far. Most patients with symptoms from degenerative spondylolisthesis do not need surgery and respond well to nonoperative care. Medications may be prescribed to help ease pain and muscle spasm. In some cases, the patient’s condition is simply monitored to see if symptoms improve.
Your doctor may ask that you rest your back by limiting your activities. This is to help decrease inflammation and calm muscle spasm. You may need to take time away from sports or other strenuous activities to give your back a chance to heal.
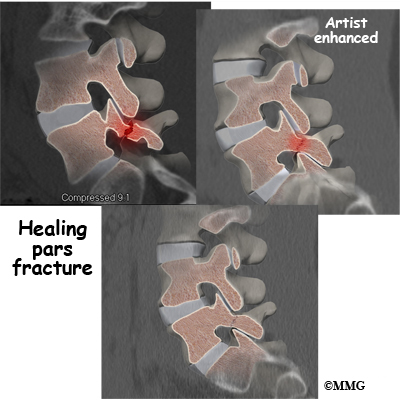
If your doctor diagnoses an acute pars fracture that has the potential to heal, it may be recommended that you wear a rigid back brace for two to three months. This usually occurs in children and teenagers who begin having back pain and see their doctor early on.

X-rays may show a fresh fracture of the pars area of the vertebra on one, or both, sides. A CT scan or bone scan may be recommended to determine if the fracture is likely to heal. If so, a brace is recommended. X-rays or a CT scan may be ordered in six to eight weeks to see if the fracture is healing. IF not, the brace will be discontinued.
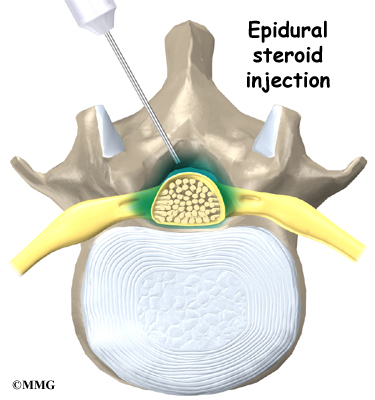
Some patients who continue to have symptoms are given an epidural steroid injection (ESI). Steroids are powerful anti-inflammatories, meaning they reduce pain and swelling. In an ESI, medication is injected into the space around the lumbar nerve roots. This area is called the epidural space. Some doctors inject only a steroid. Most doctors, however, combine a steroid with a long-lasting numbing medication. Generally, an ESI is given only when other treatments aren’t working. But ESIs are not always successful in relieving pain. If they do work, they may only provide temporary relief.
Patients often work with a physical therapist. After evaluating your condition, your therapist can assign positions and exercises to ease your symptoms. Your therapist can design an exercise program to improve flexibility in your low back and hamstrings and to strengthen your back and abdominal muscles.
The use of a stationary bike can promote aerobic conditioning and puts you in the optimal position to open the spaces where the nerve roots exit. This type if exercise program can aid in reducing the painful symptoms.
Surgery
Surgery is used when the slip is severe and when symptoms are not relieved with nonsurgical treatments. Symptoms that cause an abnormal walking pattern, changes in bowel or bladder function, or steady worsening in nerve function require surgery. Deterioration of symptoms is common in patients with a history of significant neurologic symptoms who don’t have surgery to correct the problem.
If a reasonable trial of conservative care (three months or more) does not improve things and/or your quality of life is significantly reduced, then surgery may be the next best solution. The main types of surgery for spondylolisthesis include
- laminectomy (decompression)
- posterior fusion with or without instrumentation
- posterior lumbar interbody fusion
Laminectomy
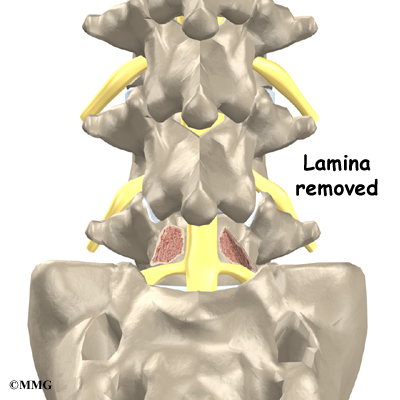
When the vertebra slips forward, the nearby nerves that exit the spine can become pinched or irritated. In addition, the size of the spinal canal in the problem area shrinks, placing pressure on the nerves inside the canal. To fix this, the lamina of the bony ring is removed to ease pressure on the nerves. The procedure to remove the lamina and release pressure on the nerves is called laminectomy. Decompression alone is usually not advised. Studies show much better results when the operation is combined with a fusion of the involved vertebrae (see below).
Related Document: A Patient’s Guide to Lumbar Laminectomy
Posterior Fusion with Instrumentation
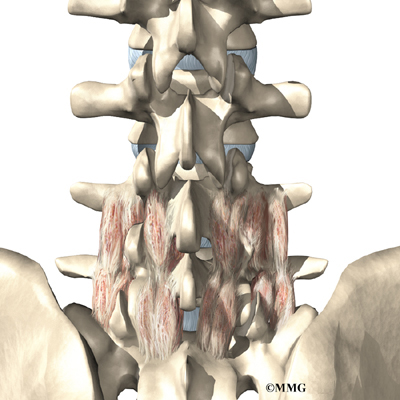
A spinal fusion is normally done immediately after laminectomy for spondylolisthesis. The fusion procedure is designed to fuse the two vertebrae into one bone and stop the slippage from worsening. The fusion is used to lock the vertebrae in place and stop movement between the vertebrae, easing mechanical pain. When combined with laminectomy surgery (mentioned earlier), fusion helps relieve nerve compression.
In this procedure, the surgeon lays small grafts of bone over the back of the problem vertebrae.

Sometimes fusion is done just with bone graft material. This is a fusion without fixation (non-instrumentation). Instrumentation is the use of metal plates or screws to stabilize the segment during healing. Most surgeons combine fusion with instrumentation to prevent the two vertebrae from moving. This protects the graft so it can heal better and faster.
Outcomes are improved when decompression is combined with fusion (compared with decompression alone). Fusion and functional improvement are even better when spinal instrumentation is used. There are fewer long-term problems with pain and pseudoarthrosis (formation of movement or false joints within the fusion).
Related Document: A Patient’s Guide to Posterior Lumbar Fusion
Posterior Lumbar Interbody Fusion
When fusion surgery is needed for mild spondylolisthesis (up to 50 percent slippage), posterior lumbar interbody fusion may be considered. In this procedure, the problem vertebrae are fused from the anterior (front) and posterior (back). Combining fusion of both portions of the spine increases the fusion surface area and improves the fusion rate. The surgeon works from the back of the spine and removes the disc between the problem vertebrae. Bone graft material is inserted from the back of the spine into the space between the two vertebrae where the disc was removed (the interbody space). The graft may be held in place with a special fusion cage that spreads and holds the vertebrae apart. Surgeons usually apply some form of instrumentation (described above) on the back of the vertebrae. In some cases, additional strips of bone graft are placed along the back surfaces of the vertebrae to be fused. This increases the mechanical strength of the spine.
Related Document: A Patient’s Guide to Posterior Lumbar Interbody Fusion
Fusion with Biologics
New materials for fusion are being developed and tested. For example, bone morphogenetic proteins (BMP) mixed with bone graft in a putty is under investigation. This substance may help reduce the need for instrumentation with fusion.
BMP helps promote faster and more bone growth in the unstable spinal segment. Studies of safety and effectiveness of this material have been very favorable so far. Without the need to harvest bone graft and place instrumentation, surgical time is much less with BMP putty. And the fusion rate is much higher with BMP alone compared with fusion alone or fusion with fixation.
Motion-Sparing Technologies
The Food and Drug Administration (FDA) is reviewing the use of devices inserted without invasive surgery to limit vertebral motion. For example, a special titanium implant has been designed to fit between the spinous processes of the vertebrae in your lower back.
These motion-sparing devices are currently used with patients who have spinal stenosis (narrowing of the spinal canal or foramen). With spondylolisthesis, the goal is to reduce the load on the disc and facets while increasing the space inside the spinal canal and foramen, thus relieving your symptoms. The vertebral segment is stabilized enough to prevent further progression of the spondylolisthesis.
Rehabilitation
What should I expect as I recover?
Nonsurgical Rehabilitation
Back pain associated with spondylolisthesis will gradually improve in up to one-third of all patients. Slippage of one vertebra over the other does not increase in this group. Worsening of symptoms is not expected in patients who don’t have neurologic symptoms at the time of diagnosis.
Nonsurgical treatment for spondylolisthesis commonly involves physical therapy. Your doctor may recommend that you work with a physical therapist a few times each week for four to six weeks. In some cases, patients may need a few additional weeks of care.
The first goal of treatment is to control symptoms. Your therapist works with you to find positions and movements that ease pain. Treatments of heat, cold, ultrasound, and electrical stimulation may be used to calm pain and muscle spasm. Patients are shown how to stretch tight muscles, especially the hamstring muscles on the back of the thigh.
As patients recover, they gradually advance in a series of strengthening exercises for the abdominal and low back muscles. Working these core muscles helps patients move easier and lessens the chances of future pain and problems.

A primary purpose of therapy is to help you learn how to take care of your symptoms and prevent future problems. You’ll be given a home program of exercises to continue improving flexibility, posture, endurance, and low back and abdominal strength. The therapist will also describe strategies you can use if your symptoms flare up.
After Surgery
Rehabilitation after surgery is more complex. Patients who have surgery for spondylolisthesis usually stay in the hospital for a few days afterward.
Some surgeons require patients to wear a rigid brace or cast for up to four months after fusion surgery for spondylolisthesis. Patients who’ve had fusion surgery for a severe slip may also be required to stay off their feet for four months.
After lumbar fusion surgery for spondylolisthesis, patients must normally wait four months before beginning a rehabilitation program. This delay is needed to give the fusion a chance to start healing. Patients typically need to attend therapy sessions for six to eight weeks and should expect full recovery to take at least 12 months.
Ideally, patients are able to return to their previous activities. However, some patients may need to modify or discontinue certain activities to avoid future problems.
When your treatment is well under way, regular visits to the therapist’s office will end. The therapist will continue to be a resource for you. But you will be in charge of doing your exercises as part of an ongoing home program.
Lumbar Disc Herniation
A Patient’s Guide to Lumbar Disc Herniation
Introduction
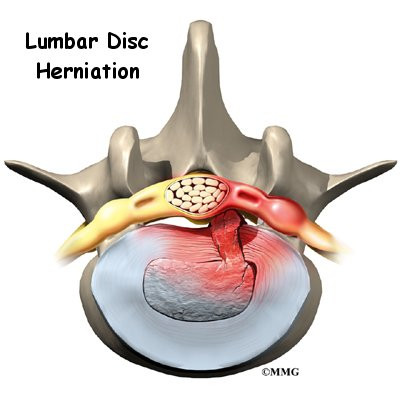
Although people often refer to a disc herniation as a slipped disc, the disc doesn’t actually slip out of place. Rather, the term herniation means that the material at the center of the disc has squeezed out of its normal space. This condition mainly affects people between 30 and 40 years old.
This guide will help you understand
- how the problem develops
- how doctors diagnose the condition
- what treatment options are available
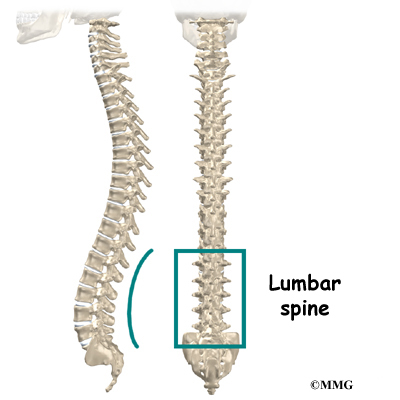
Anatomy
What parts of the spine are involved?
The human spine is formed by 24 spinal bones, called vertebrae. Vertebrae are stacked on top of one another to form the spinal column. The spinal column gives the body its form. It is the body’s main upright support. The section of the spine in the lower back is known as the lumbar spine.
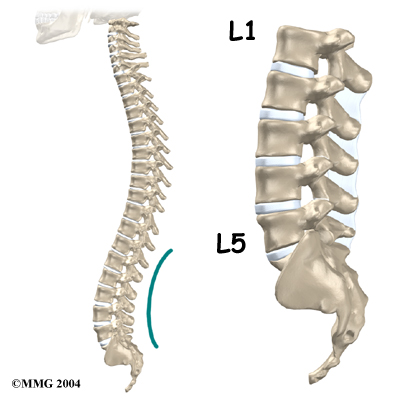
The lumbar spine is made up of the lower five vertebrae. Doctors often refer to these vertebrae as L1 to L5. These five vertebrae line up to give the low back a slight inward curve. The lowest vertebra of the lumbar spine, L5, connects to the top of the sacrum, a triangular bone at the base of the spine that fits between the two pelvic bones. Some people have an extra, or sixth, lumbar vertebra. This condition doesn’t usually cause any particular problems.
Intervertebral discs separate the vertebrae. The discs are made of connective tissue. Connective tissue is the material that holds the living cells of the body together. Most connective tissue is made of fibers of a material called collagen. These fibers help the disc withstand tension and pressure.
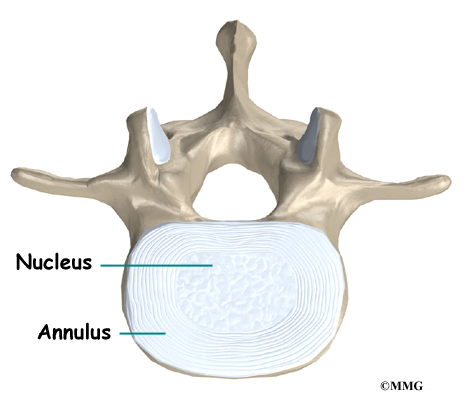
A disc is made of two parts. The center, called the nucleus, is spongy. It provides most of the disc’s ability to absorb shock. The nucleus is held in place by the annulus, a series of strong ligament rings surrounding it. Ligaments are connective tissues that attach bones to other bones.
Healthy discs work like shock absorbers to cushion the spine. They protect the spine against the daily pull of gravity. They also protect it during strenuous activities that put strong force on the spine, such as jumping, running, and lifting.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
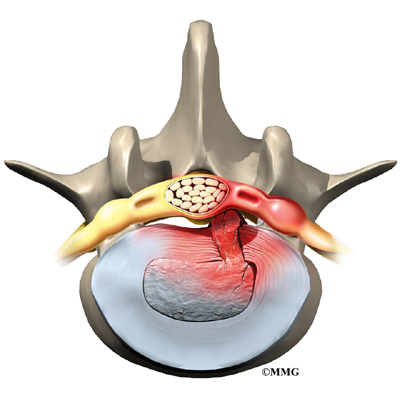
Causes
Why do I have this problem?
Herniation occurs when the nucleus in the center of the disc pushes out of its normal space. The nucleus presses against the annulus, causing the disc to bulge outward. Sometimes the nucleus herniates completely through the annulus and squeezes out of the disc.
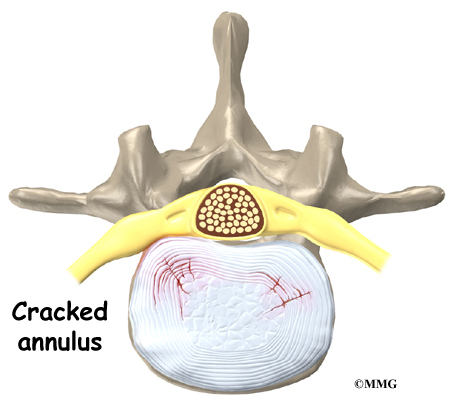
Although daily activities may cause the nucleus to press against the annulus, the body is normally able to withstand this pressure. However, as the annulus ages, it tends to crack and tear. It is repaired with scar tissue. This process is known as degeneration. Over time, the annulus weakens, and the nucleus may begin to herniate (squeeze) through the damaged annulus. At first, the pressure bulges the annulus outward. Eventually, the nucleus may herniate completely through the outer ring of the disc.
Related Document: A Patient’s Guide to Lumbar Degenerative Disc Disease
Vigorous, repetitive bending, twisting, and lifting can place abnormal pressure on the shock-absorbing nucleus of the disc. If great enough, this increased pressure can injure the annulus, leading to herniation.
A lumbar disc can also become herniated during an acute (sudden) injury. Lifting with the trunk bent forward and twisted can cause a disc herniation. A disc can also herniate from a heavy impact on the spine, such as falling from a ladder and landing in a sitting position.
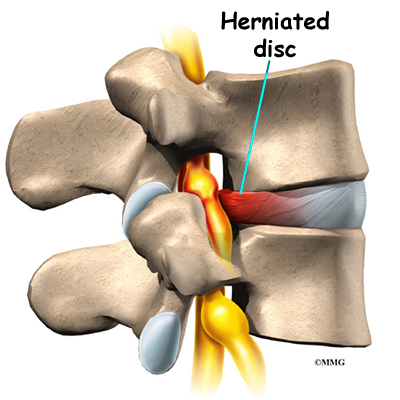
Herniation causes pain from a variety of sources. It can cause mechanical pain. This is pain that comes from the parts of the spine that move during activity, such as the discs and ligaments. Pain from inflammation occurs when the nucleus squeezes through the annulus. The nucleus normally does not come in contact with the body’s blood supply. However, a tear in the annulus puts the nucleus at risk for contacting this blood supply. When the nucleus herniates into the torn annulus, the nucleus and blood supply meet, causing a reaction of the chemicals inside the nucleus. This produces inflammation and pain. A disc herniation may also put pressure against a spinal nerve. Pressure on an irritated or damaged nerve can produce pain that radiates along the nerve. This is called neurogenic pain.
Symptoms
What does the condition feel like?
Many cases of lumbar disc herniation result from degenerative changes in the spine. The changes that eventually lead to a disc herniation produce symptoms gradually. At first, complaints may only be dull pain centered in the low back, pain that comes and goes over a period of a few years. Doctors think this is mainly from small tears in the annulus. Larger cracks in the annulus may spread pain into the buttocks or lower limbs.
When the disc herniates completely through the annulus, it generally causes immediate symptoms, with sharp pain that starts in one hip and shoots down part or all of the leg. Commonly, patients no longer feel their usual back pain, only leg pain. This is likely because painful tension on the annulus releases when the nucleus pushes completely through.
Disc herniations produce inflammation when the nucleus comes in contact with the body’s blood supply (mentioned earlier). The inflammation can be a source of throbbing pain in the low back and may spread into one or both hips and buttocks.
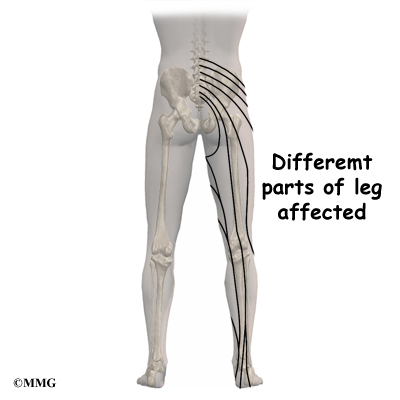
A herniated disc can press against a spinal nerve, producing symptoms of nerve compression. Nerve pain follows known patterns in the lower limbs. It can be felt on the side of the upper thigh, in the calf, or even in the foot and toes.
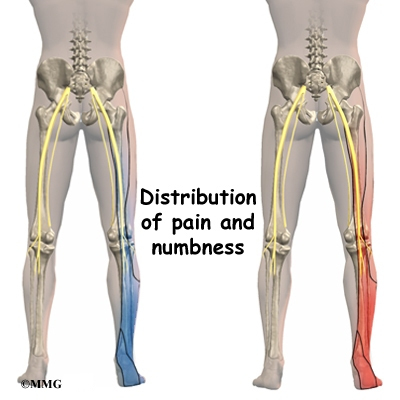
Pressure on the nerve can also cause sensations of pins, needles, and numbness where the nerve travels down the lower limbs. If this happens, a person’s reflexes slow. The muscles controlled by the nerve weaken, and sensation in the skin where the nerve goes is impaired.
Rarely, symptoms involve changes in bowel and bladder function. A large disc herniation that pushes straight back into the spinal canal can put pressure on the nerves that go to the bowels and bladder.
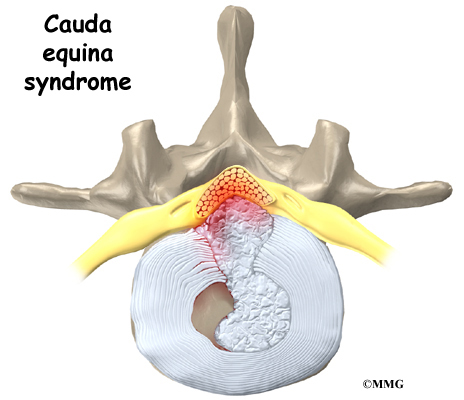
The pressure may cause low back pain, pain running down the back of both legs, and numbness or tingling between the legs in the area you would contact if you were seated on a saddle. The pressure on the nerves can cause a loss of control in the bowels or bladder. This is an emergency. If the pressure isn’t relieved, it can lead to permanent paralysis of the bowels and bladder. This condition is called cauda equina syndrome. Doctors recommend immediate surgery to remove pressure from the nerves.
Diagnosis
How do doctors diagnose the problem?
Diagnosis begins with a complete history and physical exam. Your doctor will ask questions about your symptoms and how your problem is affecting your daily activities. These will include questions about where you feel pain and whether you have numbness or weakness in your legs. Your doctor will also want to know what positions or activities make your symptoms worse or better. Doctors rely on your report of pain to get an idea which disc is causing problems and if a nerve is being squeezed.
Then the doctor examines you to determine which back movements cause pain or other symptoms. Your skin sensation, muscle strength, and reflexes are also tested.

X-rays are of minor help in diagnosing disc herniations. The discs don’t actually show up on X-rays. However, doctors can tell if the space between the vertebrae is smaller than normal. This can be an indication that wear and tear on one or more discs is causing problems. However, many peoples’ X-rays show degeneration of the discs. This is because degeneration in the discs is part of aging, like skin that wrinkles with time.
Computed tomography (a CT scan) may be ordered. This is a detailed X-ray that lets doctors see slices of the body’s tissue. The image can show if a herniated disc is putting pressure on a spinal nerve.
Doctors may combine the CT scan with myelography. To do this, a special dye is injected into the space around the spinal canal, called the the subarachnoid space. When the CT scan is performed, the dye highlights the spinal cord and nerves. The dye can improve the accuracy of a standard CT scan for diagnosing a herniated disc.
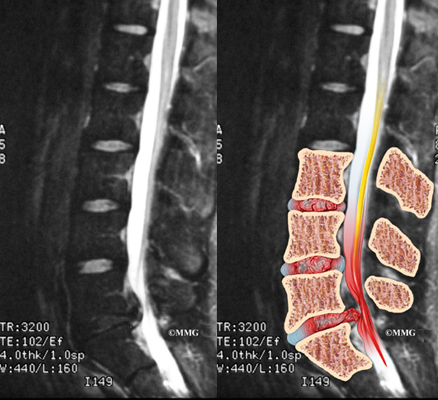
When more information is needed, your doctor may order magnetic resonance imaging (MRI). The MRI machine uses magnetic waves rather than X-rays to show the soft tissues of the body. It gives a clear picture of the discs and whether a herniation is present. Like the CT scan, this machine creates pictures that look like slices of the area your doctor is interested in. The test does not require special dye or a needle.


Doctors sometimes order a specialized X-ray test called discography. In this test, dye is injected into one or more discs. The dye is seen on X-ray and can give some information about the health of one or more discs. This test may be used when surgery is being considered to determine which disc is causing problems.
Doctors may also order electrical tests to locate more precisely which spinal nerve is being squeezed. Several tests are available to see how well the nerves are functioning, including the electromyography (EMG) test. This test measures how long it takes a muscle to work once a nerve signals it to move. The time it takes will be slower if a herniated disc has put pressure on a spinal nerve. Another test is the somatosensory evoked potential (SSEP) test. The SSEP is used to measure nerve sensations. These sensory impulses travel up the nerve, informing the body about sensations such as pain, temperature, and touch. The function of a nerve is recorded by an electrode placed over the skin in the area where the nerve travels. Doctors will often run these tests before performing surgery for a lumbar disc herniation.
Treatment
What treatment options are available?
Nonsurgical Treatment
Unless your condition is causing significant problems or is rapidly getting worse, most doctors will begin with nonsurgical treatment.
At first, your doctor may want your low back immobilized. Keeping the back still for a short time can calm inflammation and pain. This might include one or two days of bed rest. Lying on your back can take pressure off sore discs and nerves. However, most doctors advise against strict bed rest and prefer their patients to do ordinary activities using pain to gauge how much is too much. In rare cases in which bed rest is prescribed, it is usually used for a maximum of two days.
A back support belt is sometimes used for patients with lumbar disc herniation. The belt can help lower pressure inside the problem disc. Patients are encouraged to gradually discontinue wearing the support belt over a period of two to four days. Otherwise, their trunk muscles begin to rely on the belt and start to atrophy (shrink).
Doctors prescribe certain types of medication for patients with lumbar disc herniation. At first, you may be prescribed anti-inflammatory medications such as aspirin or ibuprofen. Severe symptoms that don’t go away may be treated with narcotic drugs, such as codeine or morphine. But narcotics should only be used for the first few days or weeks because they are addictive when used too much or improperly. Muscle relaxants may be prescribed if the low back muscles are in spasm. Pain that spreads down the leg is sometimes relieved with oral steroids taken in tapering dosages.
You may work with a physical therapist. Therapy treatments focus on relieving pain, improving back movement, and fostering healthy posture. A therapist can design a program to help you prevent future problems.
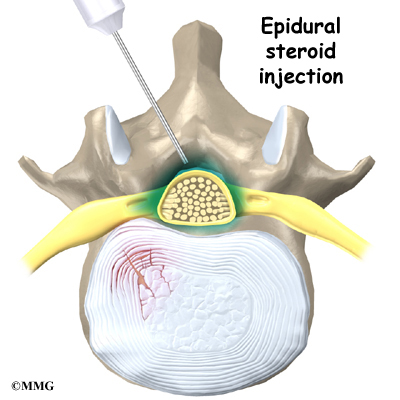
Some patients who continue to have symptoms are given an epidural steroid injection (ESI). Steroids are powerful anti-inflammatories. In an ESI, medication is injected into the space around the lumbar spinal nerves where they branch off of the spinal cord. This area is called the epidural space. Some doctors inject only a steroid. Most doctors, however, combine a steroid with a long-lasting numbing medication. Generally, an ESI is given only when other treatments aren’t working. But ESIs are not always successful in relieving pain. If they do work, they often provide only temporary relief.
Most people with a herniated lumbar disc get better without surgery. As a result, doctors usually have their patients try nonoperative treatments for at least six weeks before considering surgery. But when patients simply aren’t getting better, or if the problem is becoming more severe, surgery may be suggested.
Surgery
If the symptoms you feel are mild and there is no danger they’ll get worse, surgery is not usually recommended. However, if signs appear that pressure is building on the spinal nerves, surgery may be required, sometimes right away. The signs doctors watch for when reaching this decision include weakening in the leg muscles, pain that won’t ease up, and problems with the bowels or bladder.
Surgical treatment for lumbar disc herniation includes
- laminotomy and discectomy
- microdiscectomy
- posterior lumbar fusion

Laminotomy and Discectomy
The lamina forms a roof-like structure over the back of the spinal canal. In this procedure, a thumbnail-sized piece of the lamina is removed (laminotomy) so the surgeon can more easily take out the problem disc (discectomy). This procedure is mainly used when the herniated disc is putting pressure on a nerve and causing pain to spread down one leg.
Related Document: A Patient’s Guide to Lumbar Discectomy
Microdiscectomy
Microdiscectomy is becoming the standard surgery for lumbar disc herniation. The procedure is used when a herniated disc is putting pressure on a nerve root. It involves carefully taking out part of the problem disc (discectomy). By performing the operation with a surgical microscope, the surgeon only needs to make a very small incision in the low back. Categorized as minimally invasive surgery, this surgery is thought to be less taxing on patients. Advocates also believe that this type of surgery is easier to perform, that it prevents scarring around the nerves and joints, and that it helps patients recover more quickly.
Posterior Lumbar Fusion
Lumbar disc herniation causes mechanical pain, the type of pain caused by wear and tear in the parts of the lumbar spine. Fusion surgery is mainly used to stop movement of the painful area by joining two or more vertebrae into one solid bone. This keeps the bones and joints from moving, easing mechanical pain.
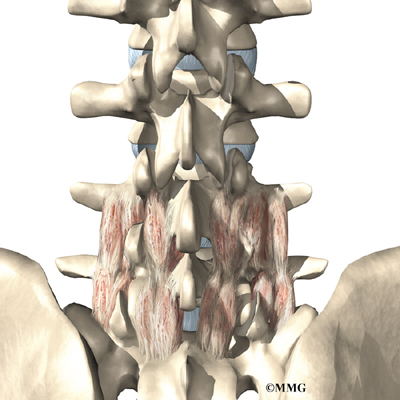
In posterior lumbar fusion, the surgeon lays small grafts of bone over the problem area on the back of the spinal column. Most surgeons will also apply metal plates and screws to prevent the problem vertebrae from moving. This protects the graft so it can heal better and faster.
Related Document: A Patient’s Guide to Posterior Lumbar Fusion
Rehabilitation
What should I expect as I recover?
Nonsurgical Rehabilitation
Even if you don’t need surgery, your doctor may recommend that you work with a physical therapist. Patients are normally seen a few times each week for four to six weeks. In severe cases, patients may need a few additional weeks of care.
The first goal of treatment is to control symptoms. Your therapist will help you find positions and movements that ease pain. Treatments of heat, cold, ultrasound, and electrical stimulation may be used in the first few sessions. Lumbar traction may also be used at first to ease symptoms of lumbar disc herniation. In addition, your therapist may use hands-on treatments such as massage or spinal manipulation. These forms of treatment are mainly used to help reduce pain and inflammation so you can resume normal activity as soon as possible.
The therapist shows you how to keep your spine safe during routine activities. You’ll learn about healthy posture and how posture relates to the future health of your spine. You’ll learn about body mechanics, how the body moves and functions during activity. Therapists teach safe body mechanics to help you protect the low back as you go about your day. This includes the use of safe positions and movements while lifting and carrying, standing and walking, and performing work duties.
Next comes a series of strengthening exercises for the abdominal and low back muscles. Working these core muscles helps patients begin moving easier and lessens the chances of future pain and problems.
Aerobic exercises such as walking or swimming are used for easing pain and improving endurance.
Your therapist will work closely with your doctor and employer to help you get back on the job as quickly as reasonably possible. You may be required to do lighter duties at first, but as soon as you are able, you’ll begin doing your normal work activities. Your therapist can do a work assessment to make sure you’ll be safe to do your job. Your therapist may suggest changes that could help you work safely, with less chance of re-injuring your back.
A primary purpose of therapy is to help you learn how to take care of your symptoms and prevent future problems. You’ll be given a home program of exercises to continue improving flexibility, posture, endurance, and low back and abdominal strength. The therapist will also discuss strategies you can use if your symptoms flare up.
After Surgery
Rehabilitation after surgery is more complex. Some patients leave the hospital shortly after surgery. However, some surgeries require patients to stay in the hospital for a few days. Patients who stay in the hospital may visit with a physical therapist in the hospital room soon after surgery. The treatment sessions help patients learn to move and do routine activities without putting extra strain on the back.
During recovery from surgery, patients should follow their surgeon’s instructions about wearing a back brace or support belt. They should be cautious about overdoing activities in the first few weeks after surgery.
Many surgical patients need physical therapy outside of the hospital. They see a therapist for one to three months, depending on the type of surgery. At first, therapists may use treatments such as heat or ice, electrical stimulation, massage, and ultrasound to help calm pain and muscle spasm. They provide reassurance to help patients deal with fear and apprehension about pain. Then they teach patients how to move safely with the least strain on the healing back. Exercises are used to improve flexibility, strength, and endurance.
When your treatment is well under way, regular visits to the therapist’s office will end. The therapist will continue to be a resource for you. But you will be in charge of doing your exercises as part of an ongoing home program.
Anterior Lumbar Fusion with Cages
A Patient’s Guide to Anterior Lumbar Fusion with Cages
Introduction
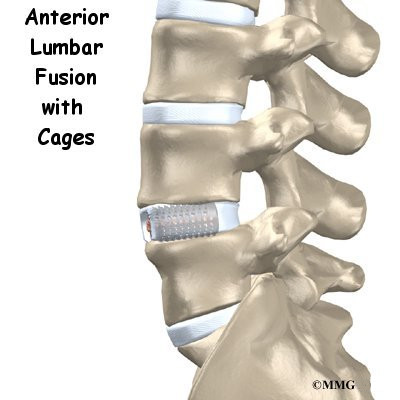
Anterior lumbar fusion is an operation done on the front (the anterior region) of the lower spine. Fusion surgery helps two or more bones grow together into one solid bone. Fusion cages are new devices, essentially hollow screws filled with bone graft, that help the bones of the spine heal together firmly. Surgeons use this procedure when patients have symptoms from disc degeneration, disc herniation, or spinal instability.
This guide will help you understand
- why the procedure becomes necessary
- what surgeons hope to achieve
- what to expect during your recovery
Anatomy
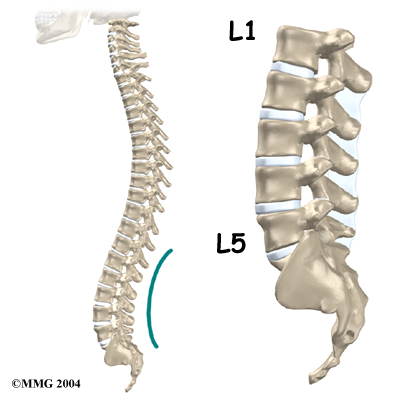
What parts of the spine are involved?
Since the surgeon needs to reach the front of the spine, this operation is done through the abdomen. The main structures involved in this procedure are the vertebral bodies and the intervertebral discs.
The vertebral bodies are the large blocks of bone that make up the front section of each vertebra. The intervertebral discs are the cushions between each pair of vertebrae.
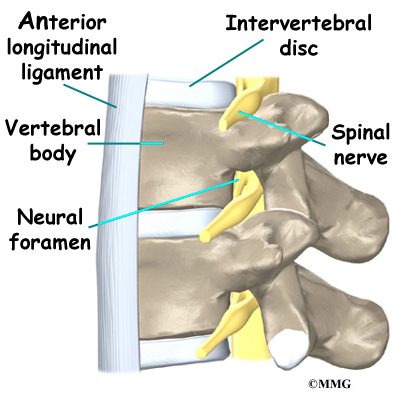
The fusion cages help separate the vertebral bodies, taking pressure off the spinal nerves wherethey travel from the spinal canal through openings called the neural foramen.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Rationale
What do surgeons hope to achieve?
In most cases, this procedure is used to stop symptoms from lumbar disc disease. The intervertebral discs in the spine degenerate as a natural part of aging. Daily wear and tear and certain types of vibration can also speed up degeneration in the spine. In addition, strong evidence suggests that smoking speeds up degeneration of the spine. Scientists have also found links among family members, showing that genetics plays a role in how fast these changes occur. When degeneration occurs, a problem disc begins to collapse, and the space decreases between the vertebrae.
Related Document: A Patient’s Guide to Lumbar Degenerative Disc Disease
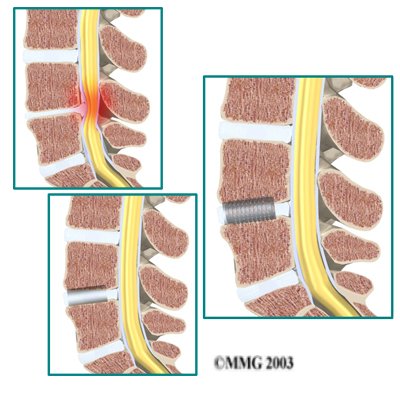
When this happens, the opening around the spinal nerves (the neural foramen) narrows and may begin to put pressure on the nerves. The long ligaments in the spine slacken. They may even buckle and put pressure on the spinal nerves. The outer rings of the disc, the annulus, weaken and develop small cracks. The nucleus in the center of the disc presses on the weakened annulus and may actually squeeze through the annulus and press on ligaments or nerves. Fragments of the disc that press against the outer annulus and spinal nerves can be a source of pain, numbness, and weakness. Pressure on the spinal nerves can also produce problems with the bowels and bladder, requiring emergency surgery.
View animation of degeneration
A fusion operation can reduce or eliminate the pain caused by a problem disc. If the fusion is successful, the vertebrae that are fused together no longer move against one another. Instead, they move together as one unit. This prevents the disc from causing pain.
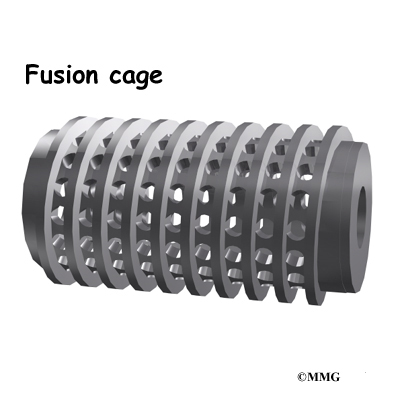
Fusion cages are also designed to separate and hold the vertebrae apart. Enlarging the space between two vertebrae widens the opening of the neural foramina, taking pressure off the spinal nerves that pass through them. Also, the extra space pulls taut the ligaments inside the spinal canal so they don’t buckle into the spinal canal.
View animation of regaining disc height
Fusion cages are most commonly made of metal, graphite, or bone. Many of these cages are shaped like cylinders. A few are rectangular in shape. They are usually threaded like a screw on the outside and hollow on the inside. The main purpose of the cage, regardless of the shape or material, is to hold the two vertebrae apart while the fusion becomes solid.
The surgeon packs the hollow center of the cage with bone. The graft is commonly taken from another part of the body, usually the top of the pelvis bone. Bone taken from another part of your own body is called an autograft. There is a risk of pain, infection, or weakness in the area where the graft is taken.
A new method to avoid this problem is with a bone graft substitute. By using gene therapy, scientists have produced bone graft substitutes called growth factors. These growth factors are natural proteins found in the human body. Genetic engineers have been able to clone proteins known as bone morphogenic proteins (BMPs). These proteins are then made available as powder, small particles, or chips. Hormones that circulate in the bloodstream act on the BMP molecules, causing them to build new bone tissue.
The growth factor that is approved for lumbar fusion with titanium cages is BMP-2. Substituting BMP-2 for an autograft eliminates the complications that go with harvesting autograft material from the patient’s own body. This allows for shorter operation times, less loss of blood during surgery, and quicker recovery times for patients. New research shows that BMP-2 is at least as good as, and maybe even better than, autograft for anterior lumbar fusion with cages.
The surgeon packs the hollow center of the fusion cages with bone graft, either in the form of an autograft or bone graft substitute. Two cages are placed side by side within the disc. The cages spread the vertebrae apart, and the threads bind the vertebrae to keep them from moving. After implanting the cages, most surgeons attach metal hardware on the vertebrae to rigidly lock them in place. This helps the bone graft heal, fusing the vertebrae together.
Once the bones fuse, they are prevented from moving against one another. This helps relieve the mechanical pain, which occurs in the moving parts of the back. Fusion also prevents additional wear and tear on the structures inside the section that was fused. By fusing the bones together, surgeons hope to reduce future problems at the spinal segment.
Preparations
How will I prepare for surgery?
The decision to proceed with surgery must be made jointly by you and your surgeon. You should understand as much about the procedure as possible. If you have concerns or questions, talk to your surgeon.
Once you decide on surgery, your surgeon may suggest a complete physical examination by your regular doctor. This exam helps ensure that you are in the best possible condition to undergo the operation.
On the day of your surgery, you will probably be admitted to the hospital early in the morning. You shouldn’t eat or drink anything after midnight the night before.
Surgical Procedure
What happens during the operation?
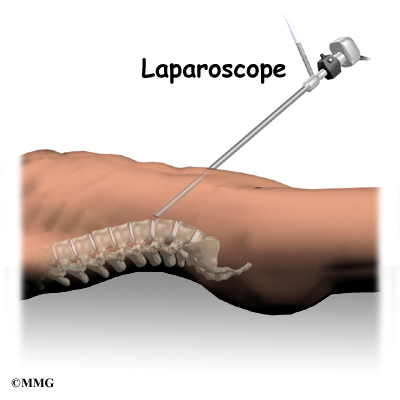
Traditionally, this operation requires a sizeable abdominal incision. Recently, however, surgeons have begun using a laparoscope in this operation. A laparoscope is a small television camera that lets the surgeon see inside the abdominal cavity to perform the operation. Several much smaller abdominal incisions are needed in the laparoscopic method. The smaller incisions allow patients to begin moving sooner and healing faster. However, performing anterior lumbar fusion with a laparoscope is difficult. It isn’t the right choice for all fusion surgeries.
Patients are positioned on their backs with a pad placed under the low back. They are given general anesthesia to put them to sleep. As they sleep, their breathing may be assisted with a ventilator. A ventilator is a device that controls and monitors the flow of air to the lungs.
In the traditional method, an incision is made through one side of the abdomen. Organs and blood vessels are gently moved aside to expose the front of the lumbar spine.
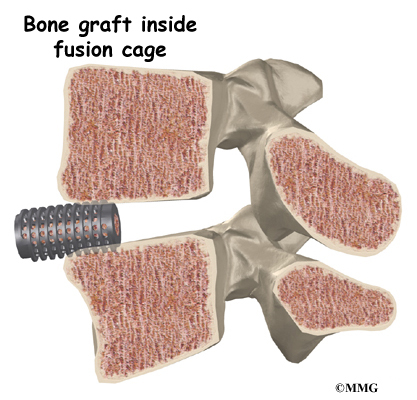
The problem disc is located with a fluoroscope, a special X-ray that shows images on a TV screen. The surgeon drills two large holes horizontally through the front of the disc. The fusion cages are sized to fit into the newly drilled holes. Bone graft may be taken from the top of the pelvis. The other option is for the surgeon to use a bone graft substitute. The bone graft material is packed into the hollow cages. Then the surgeon screws the cages into the holes in the disc. The threads of the cages clinch the vertebrae above and below, holding them rigidly in place. The fluoroscope is used to check the position and fit of the cages.
As mentioned earlier, the surgeon may also fix the vertebrae in place using metal screws or plates. One option is screwing a strap of metal across the front of the spine. A second method involves additional surgery through the low back. This may be done on the same day or during a later surgery. Metal plates or screws applied through the back of the spine lock the two vertebrae and prevent them from moving. This protects the graft so it can heal better and faster.
Related Document: A Patient’s Guide to Posterior Lumbar Fusion
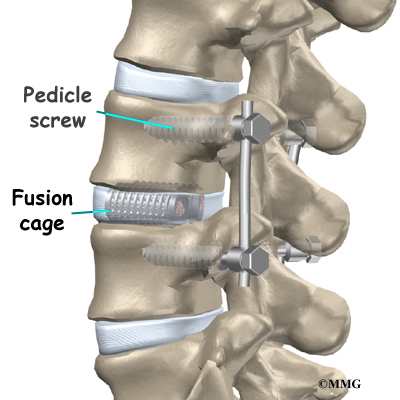
A drainage tube may be placed in the wound. The muscles and soft tissues are put back in place, and the skin is stitched together. The surgeon may place the patient in a rigid brace.
The threaded cages rigidly connect the vertebrae above and below. Small openings in the surface of the cages allow the bone graft inside to contact the surfaces of both vertebrae. As the new bone inside the cages heals to the nearby vertebrae, the two vertebrae become rigidly fused into one solid bone.
Complications
What might go wrong?
As with all major surgical procedures, complications can occur. Some of the most common complications following anterior lumbar fusion with cages include
- problems with anesthesia
- thrombophlebitis
- infection
- nerve damage
- blood vessel damage
- problems with the graft or hardware
- nonunion
- ongoing pain
This is not intended to be a complete list of the possible complications.
Problems with Anesthesia
Problems can arise when the anesthesia given during surgery causes a reaction with other drugs the patient is taking. In rare cases, a patient may have problems with the anesthesia itself. In addition, anesthesia can affect lung function because the lungs don’t expand as well while a person is under anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Thrombophlebitis (Blood Clots)
View animation of pulmonary embolism
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can occur after any operation. It occurs when the blood in the large veins of the leg forms blood clots. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lung, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Most surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective is getting you moving as soon as possible. Two other commonly used preventative measures include
- pressure stockings to keep the blood in the legs moving
- medications that thin the blood and prevent blood clots from forming
Infection
Infection following spine surgery is rare but can be a very serious complication. Some infections may show up early, even before you leave the hospital. Infections on the skin’s surface usually go away with antibiotics. Deeper infections that spread into the bones and soft tissues of the spine are harder to treat. They may require additional surgery to treat the infected portion of the spine.
Nerve Damage
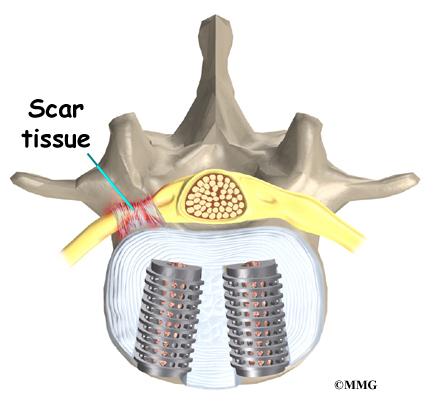
Any surgery that is done near the spinal canal can potentially cause injury to the spinal cord or spinal nerves. Injury can occur from bumping or cutting the nerve tissue with a surgical instrument, from swelling around the nerve, or from the formation of scar tissue. An injury to the spinal cord or spinal nerves can cause muscle weakness and a loss of sensation to the areas supplied by the nerve.
Blood Vessel Damage
The abdominal aorta (the largest artery in the body) and the large veins that accompany it run in front of the spine as they split to run to each leg. These vessels must be moved aside to perform the anterior cage procedure. Because of this, the vessels may be injured, causing bleeding. When the procedure is performed using the laparoscope, too much bleeding may require opening the abdomen with a larger incision to repair the injured vessels.
Problems with the Graft or Hardware
Fusion surgery with cages requires bone grafting. The graft is commonly taken from the top rim of the pelvis (autograft). As mentioned earlier, there is a risk of pain, infection, or weakness in the area where the graft is taken. These risks are avoided when a bone graft substitute, such as BMP-2, is used in place of an autograft.
After the cages are in place, the surgeon checks their position before completing the surgery. However, the cages may shift slightly soon after surgery to the point that they are no longer able to hold the spine stable. Abnormal or excessive loads on the spine, for example from heavy lifting or carrying or from the impact of jumping from a high surface, can cause the cages to collapse. This shifting or collapsing of the cages can cause injury to the nearby tissues. If this happens, a second surgery may be needed to replace the cages and to apply additional instrumentation to lock the spine firmly in place.
Hardware can also cause problems. Screws or pins may loosen and irritate the nearby soft tissues. Also, the metal plates can sometimes break. If this happens, the surgeon may suggest another surgery either to take out the hardware or to add more hardware to solve the problem.
Nonunion
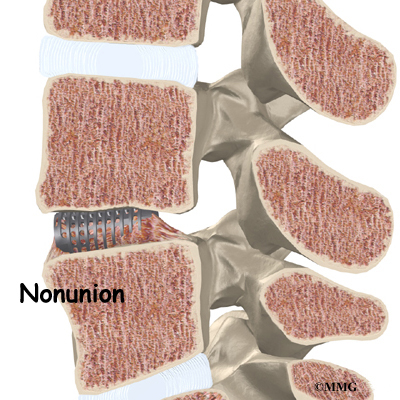
Sometimes the bones do not fuse as planned. This is called a nonunion, or pseudarthrosis. (The term pseudarthrosis means false joint.) When more than one level of the spine is fused at one time, there is a greater chance that nonunion will occur. Fusion of more than one level means two or more consecutive discs are removed and replaced with bone graft. If the joint motion from a nonunion causes pain, you may need a second operation.
In the second procedure, the surgeon may have to replace the cages. Metal plates and screws may also be added to rigidly secure the bones so they will fuse.
Ongoing Pain
Anterior lumbar fusion with cages is a complex surgery. Not all patients get complete pain relief with this procedure. As with any surgery, you should expect some pain afterward. If the pain continues or becomes unbearable, talk to your surgeon about treatments that can help control your pain.
After Surgery
What happens after surgery?
Patients are sometimes placed in a rigid body brace after surgery. This brace may not be needed if the surgeon attached metal hardware to the spine during the surgery.
Patients usually stay in the hospital after surgery for up to one week. During this time, a physical therapist helps patients learn safe ways to move, dress, and do activities without putting extra strain on the back. Patients may be instructed to use a walker for the first day or two. Before going home, patients are shown how to control pain and avoid problems.
Patients are able to return home when their medical condition is stable. However, they are usually required to keep their activities to a minimum in order to give the graft time to heal. Patients are cautioned against bending forward, lifting, twisting, driving, and prolonged sitting for up to six weeks. Activities and exercises that cause the spine to bend back place hazardous stress on the cages and should be avoided for at least six months. Outpatient physical therapy usually begins a minimum of six weeks after the date of surgery.
Rehabilitation
What should I expect as I recover?
Rehabilitation after anterior lumbar fusion with cages can be a slow process. Many surgeons prescribe outpatient physical therapy beginning a minimum of six weeks after surgery. This delay is needed to make sure the fusion is taking. You will probably need to attend therapy sessions for two to three months, and you should expect full recovery to take up to eight months. However, therapy can usually progress faster for patients who had fusion with instrumentation.
At first, treatments help control pain and inflammation. Ice and electrical stimulation treatments are commonly used to help with these goals. Your therapist may also use massage and other hands-on techniques to ease muscle spasm and pain.
Active treatments are slowly added. These include exercises for improving heart and lung function. Short, slow walks are generally safe to start with. Swimming and use of a stairclimbing machine are helpful in the later phases of treatment. Therapists also teach specific exercises to help tone and control the muscles that stabilize the low back.
Your therapist also works with you on how to move and do activities. This form of treatment, called body mechanics, helps you develop new movement habits. This training helps you keep your back in safe positions as you go about your work and daily activities. Training includes positions you use when sitting, lying, standing, and walking. You’ll also work on safe body mechanics with lifting, carrying, pushing, and pulling.
As your condition improves, the therapist tailors your program to help prepare you to go back to work. Some patients are not able to go back to a previous job that requires strenuous tasks. Your therapist may suggest changes in job tasks that enable you to go back to your previous job or to do alternate forms of work. You’ll learn to do these tasks in new ways that keep your back safe and free of strain.
Before your therapy sessions end, your therapist will teach you ways to avoid future problems.
Lumbar Facet Joint Arthritis
A Patient’s Guide to Lumbar Facet Joint Arthritis
Introduction
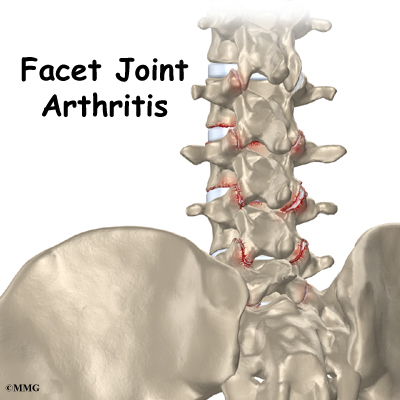
Arthritis of the lumbar facet joints can be a source of significant low back pain. Aligned on the back of the spinal column, the facet joints link each vertebra together. Articular cartilage covers the surfaces where these joints meet. Like other joints in the body that are covered with articular cartilage, the lumbar facet joints can be affected by arthritis.
This guide will help you understand
- how the problem develops
- how doctors diagnose the condition
- what treatment options are available
Anatomy

What part of the back is involved?
The human spine is made up of 24 spinal bones, called vertebrae. Vertebrae are stacked on top of one another to create the spinal column. The spinal column gives the body its form. It is the body’s main upright support.
The back portion of the spinal column forms a bony ring. When the vertebrae are stacked on top of each other, these bony rings create a hollow tube. This tube, called the spinal canal, surrounds the spinal cord as it passes through the spine. Just as the skull protects the brain, the bones of the spinal column protect the spinal cord.
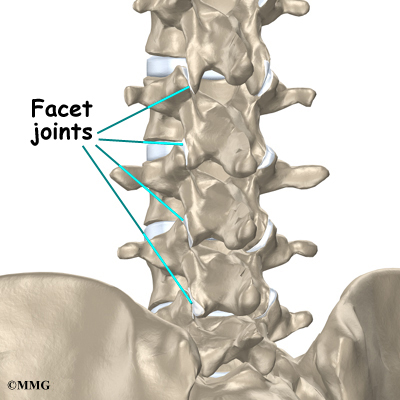
Between the vertebrae of each spinal segment are two facet joints. The facet joints are located on the back of the spinal column. There are two facet joints between each pair of vertebrae, one on each side of the spine. A facet joint is made of small, bony knobs that line up along the back of the spine. Where these knobs meet, they form a joint that connects the two vertebrae. The alignment of the facet joints of the lumbar spine allows freedom of movement as you bend forward and back.
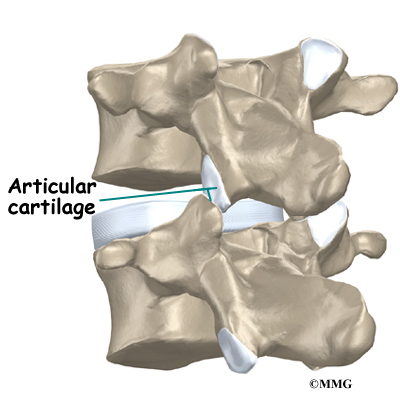
The surfaces of the facet joints are covered by articular cartilage. Articular cartilage is a smooth, rubbery material that covers the ends of most joints. It allows the bone ends to move against each other smoothly, without friction.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Causes
Why do I have this problem?
Normally, the facet joints fit together snugly and glide smoothly, without pressure. If pressure builds where the joint meets, the cartilage on the joint surfaces wears off, or erodes.
Each segment in the spine has three main points of movement, the intervertebral disc and the two facet joints. Injury or problems in any one of these structures affects the other two. As a disc thins with aging and from daily wear and tear, the space between two spinal vertebrae shrinks. This causes the facet joints to press together.
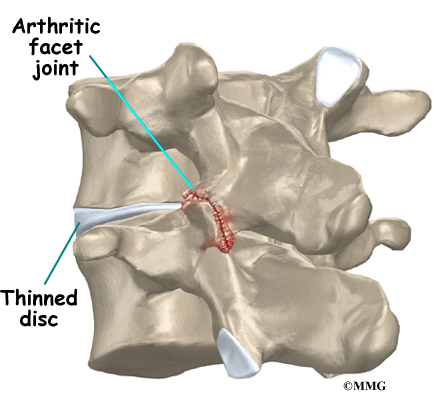
Facet joints can also become arthritic due to a back injury earlier in life. Fractures, torn ligaments, and disc problems can all cause abnormal movement and alignment, putting extra stress on the surfaces of the facet joints.
The body responds to this extra pressure by developing bone spurs. As the spurs form around the edges of the facet joints, the joints become enlarged. This is called hypertrophy. Eventually, the joint surfaces become arthritic. When the articular cartilage degenerates, or wears away, the bone underneath is uncovered and rubs against bone. The joint becomes inflamed, swollen, and painful.
View animation of facet arthritis
Facet joint arthritis develops slowly over a long period of time. This is partly because spinal degeneration in later life is the main cause of facet joint arthritis. Symptoms rarely develop immediately when degeneration is causing the problems. However, rapid movements, heavy twisting, or backward motions in the low back can injure a facet joint, leading to immediate symptoms.
Symptoms
What does the condition feel like?
Pain from facet joint arthritis is usually worse after resting or sleeping. Also, bending the trunk sideways or backward usually produces pain on the same side as the arthritic facet joint. For example, if you lie on your stomach on a flat surface and raise your upper body, you hyperextend the spine. This increases pressure on the facet joints and can cause pain if there is facet joint arthritis.
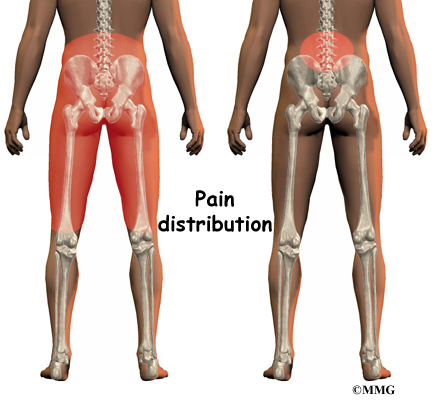
Pain may be felt in the center of the low back and can spread into one or both buttocks. Sometimes the pain spreads into the thighs, but it rarely goes below the knee. Numbness and tingling, the symptoms of nerve compression, are usually not felt because facet arthritis generally causes only mechanical pain. Mechanical pain comes from abnormal movement in the spine.
However, symptoms of nerve compression can sometimes occur at the same time as the facet joint pain. The arthritis can cause bone spurs at the edges of the facet joint. These bone spurs may form in the opening where the nerve root leaves the spinal canal. This opening is called the neural foramen. If the bone spurs rub against the nerve root, the nerve can become inflamed and irritated. This nerve irritation can cause symptoms where the nerve travels. These symptoms may include numbness, tingling, slowed reflexes, and muscle weakness.
Diagnosis
How do doctors diagnose the problem?
Diagnosis begins with a complete history and physical examination. Your doctor will ask questions about your symptoms and how your problem is affecting your daily activities. This will include questions about where you feel pain and if you have numbness or weakness in your legs. Your doctor will also want to know what positions or activities make your symptoms worse or better.
Then the doctor performs a physical exam to determine which back movements cause pain or other symptoms. Your skin sensation, muscle strength, and reflexes are also tested.
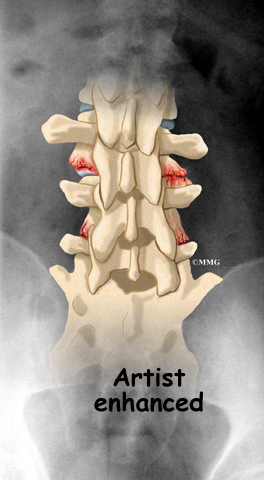
X-rays can show if there are problems in the bone tissue in and near the facet joints. The images can show if degeneration has caused the space between the vertebrae to collapse and may show if bone spurs have developed near the facet joints.
When more information is needed, your doctor may order magnetic resonance imaging (MRI). The MRI machine uses magnetic waves rather than X-rays to show the soft tissues of the body. This test gives a clear picture of the facet joints to see whether they are enlarged or swollen. This machine creates pictures that look like slices of the area your doctor is interested in. The test does not require dye or a needle.
A computed tomography (CT) scan may be ordered. This is a detailed X-ray that lets your doctor see slices of bone tissue. The image can show whether the surface of the joint has eroded and whether bone spurs have developed.

A diagnostic injection may be used to locate the source of pain. The doctor uses a long needle to inject a local anesthetic (numbing medication) into either the joint or into the nerve that goes to the joint. The doctor watches the needle on a fluoroscope to make sure it reaches the correct spot. A fluoroscope is a special X-ray television that allows the doctor to see your spine and the needle as it moves. Once the doctor is sure the needle is in the right place, the medicine and a special dye are injected. The doctor watches the dye to make sure the medication is correctly placed. The results from the injection help the doctor make the diagnosis. If pain goes away, it helps confirm the source of pain.
Treatment Options
What treatment options are available?
Nonsurgical Treatment
Facet joint arthritis is mainly treated nonsurgically. At first, doctors may prescribe a short period of rest, one to two days at most, to calm inflammation and pain. Patients may find added relief by curling up to sleep on a firm mattress or by lying back with their knees bent and supported. These positions take pressure off the facet joints.
Your doctor may prescribe anti-inflammatory medication, such as a nonsteroidal anti-inflammatory drug (NSAID) or aspirin. Muscle relaxants are occasionally used to calm muscles that are in spasm. Oral steroid medicine in tapering dosages may also be prescribed for pain.
Patients often work with a physical therapist. By evaluating a patient’s condition, the therapist can assign positions and exercises to ease symptoms. The therapist may recommend traction. Traction is a common treatment for this condition. It gently stretches the low back and takes pressure off the facet joints. The therapist may also prescribe strengthening and aerobic exercises. Strengthening exercises focus on improving the strength and control of the back and abdominal muscles. Aerobic exercises are used to improve heart and lung health and increase endurance in the spinal muscles. Stationary biking offers a good aerobic treatment and keeps the spine bent slightly forward, a position that gives relief to many patients with lumbar facet joint arthritis.
Patients who still have pain after trying various treatments may require injections into the facet joint or the small nerves that go to the joint. An anesthetic is used to block pain coming from the facet joint. The procedure to inject the medication into the joint is similar to the diagnostic injection described earlier. A steroid medication is occasionally used instead of the anesthetic. There is no strong evidence that these injections work. However, they seem to have some good short-term results with few side effects, so they shouldn’t be abandoned completely. Doctors often have their patients resume physical therapy treatments following an injection.
Related Document: A Patient’s Guide to Facet Joint Injections
Surgery
People with facet joint arthritis rarely need surgery. However, facet joint arthritis is a primary source of chronic low back pain about 15 percent of the time. After trying other types of treatment, some of these patients may eventually require surgery. There are several types of surgery for facet joint arthritis. The two primary operations are
- facet rhizotomy
- posterior lumbar fusion
Facet Rhizotomy
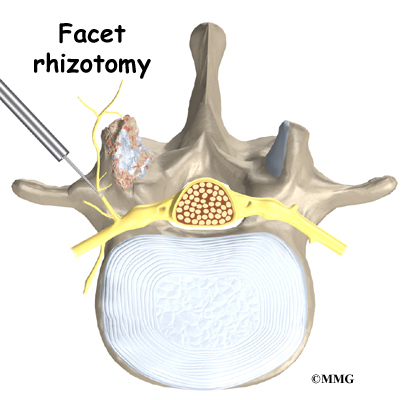
Rhizotomy describes a surgical procedure in which a nerve is purposely cut or destroyed. Facet rhizotomy involves severing one of the small nerves that goes to the facet joint. The intent of the procedure is to stop the transmission of pain impulses along this nerve. The nerve is identified using a diagnostic injection (described earlier). Then the surgeon inserts a large, hollow needle through the tissues in the low back. A special probe is inserted through the needle, and a fluoroscope is used to guide the probe toward the nerve. The probe is slowly heated until the nerve is severed.
Posterior Lumbar Fusion
Facet joint arthritis mainly causes mechanical pain, the type of pain caused by wear and tear in the parts of the lumbar spine. Posterior lumbar fusion for facet joint arthritis is mainly used to stop movement of the painful joints by joining two or more vertebrae into one solid bone (fusion). This keeps the bones and painful facet joints from moving.
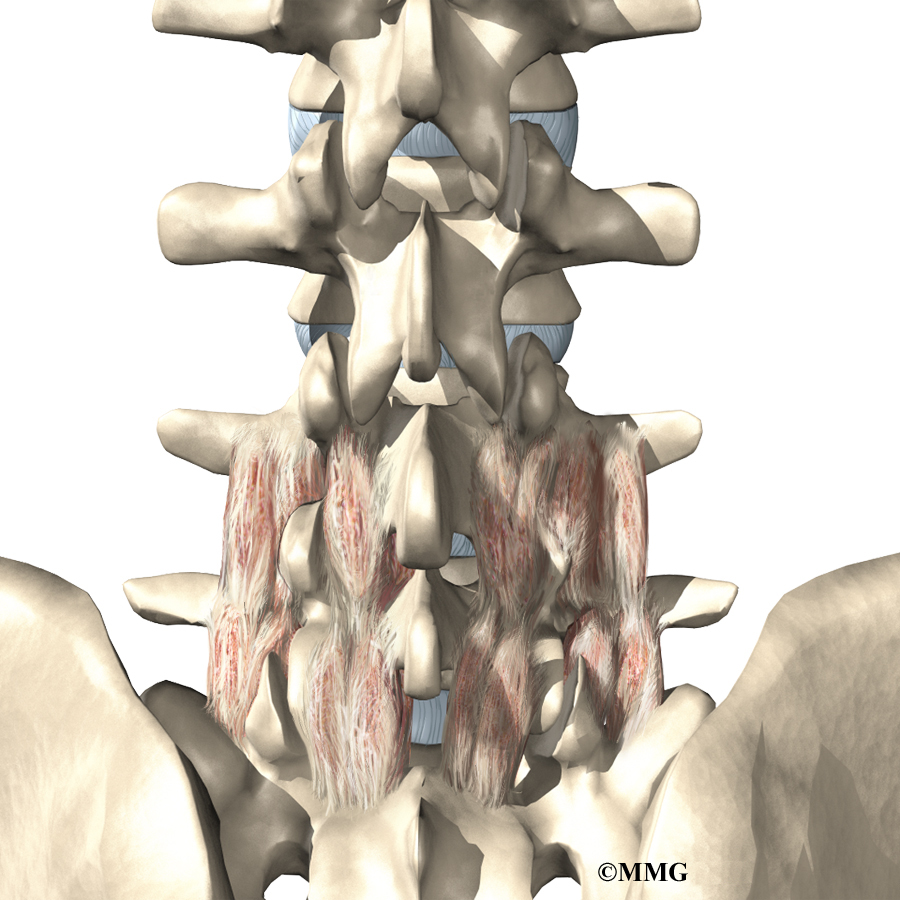
In this procedure, the surgeon lays small grafts of bone over the back of the spine. Most surgeons will also apply metal plates and screws to prevent the two vertebrae from moving. This protects the graft so it can heal better and faster.
Related Document: A Patient’s Guide to Posterior Lumbar Fusion
Rehabilitation
Nonsurgical Rehabilitation
Even if you don’t need surgery, your doctor may recommend that you work with a physical therapist. Patients are normally seen a few times each week for four to six weeks. In severe and chronic cases, patients may need a few additional weeks of care.
Therapists create programs to help patients regain back movement, strength, endurance, and function. Treatments for facet joint arthritis often include lumbar traction, described earlier. Hands-on treatments such as massage and specialized forms of soft-tissue mobilization may be used initially. They are used to help patients begin moving with less pain and greater ease.
Spinal manipulation can sometimes provide short-term relief of pain from facet arthritis. Commonly thought of as an adjustment, spinal manipulation stretches the tissues surrounding the facet joint and helps reset the sensitivity of the spinal nerves and muscles. It involves a high-impulse stretch of the spinal joints and is characterized by the sound of popping as the stretch is done. However, it doesn’t seem to provide effective long-term help when used routinely for chronic conditions.
Patients are shown how to improve strength and coordination in the abdominal and low back muscles. Therapists can also evaluate their patients’ workstations or the way they use they use their bodies when they do their activities.
After Surgery
Outpatient physical therapy is usually prescribed only for patients who have extra pain or show significant muscle weakness and deconditioning.
Patients usually don’t require physical therapy after facet rhizotomy. Surgeons may prescribe a short period of therapy when patients have lost muscle tone in their back and abdominal muscles, when they have problems controlling pain, or when they need guidance about returning to work.
If patients require formal rehabilitation after facet rhizotomy, they will probably only need to attend sessions for two to four weeks. They should expect full recovery to take up to three months.
Patients who have had lumbar fusion surgery normally need to wait at least six weeks before beginning a rehabilitation program. They typically need to attend therapy sessions for six to eight weeks and should expect full recovery to take up to six months.
During therapy after surgery, the therapist may use treatments such as heat or ice, electrical stimulation, massage, and ultrasound to help calm pain and muscle spasm. Then patients begin learning how to move safely with the least strain on the healing back.
As the rehabilitation program evolves, patients do more challenging exercises. The goal is to safely advance strength and function.
As the therapy sessions come to an end, the therapist helps patients get back to the activities they enjoy. Ideally, patients are able to resume normal activities. They may need guidance on which activities are safe or how to change the way they go about their activities.
When treatment is well under way, regular visits to the therapist’s office will end. The therapist will continue to be a resource. But patients are in charge of doing their exercises as part of an ongoing home program.
Lumbar Discectomy
A Patient’s Guide to Lumbar Discectomy
Introduction
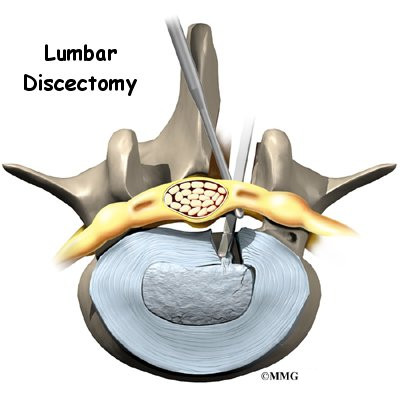
Lumbar discectomy is a surgical procedure to remove part of a problem disc in the low back. The discs are the pads that separate the vertebrae. This procedure is commonly used when a herniated, or ruptured, disc in the low back is putting pressure on a nerve root.
This guide will help you understand
- what surgeons hope to achieve
- what happens during surgery
- what to expect as you recover
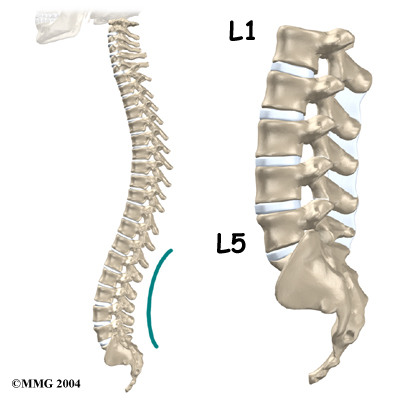
Anatomy
What parts of the spine and low back are involved?
Surgeons perform lumbar discectomy surgery through an incision in the low back. This area is known as the posterior region of the low back. The main structure involved is the intervertebral disc, which acts as a cushion between each pair of vertebrae. The two main parts of the disc are the annulus and the nucleus.
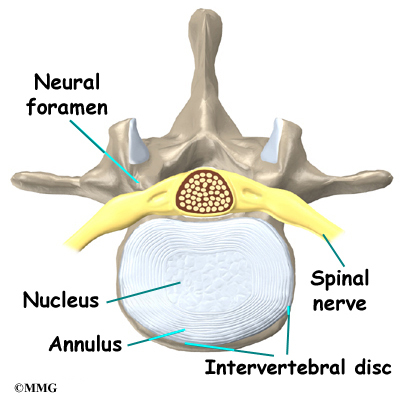
The lamina bone forms the protective covering over the back of the spinal cord. During surgery, this section of bone is removed over the problem disc. The surgeon also checks the spinal nerves where they travel from the spinal canal through the neural foramina. The neural foramina are small openings on each side of the vertebra. Nerves that leave the spine go through the foramina, one on the left and one on the right.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Rationale
What do surgeons hope to achieve?
Lumbar discectomy can alleviate symptoms from a herniated disc in the low back. The main goal of discectomy surgery is to remove the part of the disc that is putting pressure on a spinal nerve root. Taking out the injured portion of the disc also reduces chances that the disc will herniate again.
These goals can be achieved using a traditional procedure, called laminotomy and discectomy, or with a newer method called microdiscectomy. The traditional method requires a larger incision and tends to require a longer time to heal.
Microdiscectomy is becoming the standard surgery for lumbar disc herniation. Since the surgeon performs the operation with a surgical microscope, he or she needs to make only a very small incision in the low back. Categorized as minimally invasive surgery, this surgery is thought to be less taxing on patients. Advocates also believe that this type of surgery is easier to perform, prevents scarring around the nerves and joints, and helps patients recover more quickly.
Related Document: A Patient’s Guide to Lumbar Disc Herniation
Preparations
How will I prepare for surgery?
The decision to proceed with surgery must be made jointly by you and your surgeon. You should understand as much about the procedure as possible. If you have concerns or questions, you should talk to your surgeon.
Once you decide on surgery, your surgeon may suggest a complete physical examination by your regular doctor. This exam helps ensure that you are in the best possible condition to undergo the operation.
On the day of your surgery, you will probably be admitted to the hospital early in the morning. You shouldn’t eat or drink anything after midnight the night before.
Surgical Procedure
What happens during the operation?
Patients are given a general anesthesia to put them to sleep during most spine surgeries. As you sleep, your breathing may be assisted with a ventilator. A ventilator is a device that controls and monitors the flow of air to the lungs.
Some surgeons have begun using spinal anesthesia in place of general anesthesia. Spinal anesthesia is injected in the low back into the space around the spinal cord. This numbs the spine and lower limbs. Patients are also given medicine to keep them sedated during the procedure.
Discectomy surgery is usually done with the patient kneeling face down in a special frame. The frame supports the patient so the abdomen is relaxed and free of pressure. This position lessens blood loss during surgery and gives the surgeon more room to work.
The two main discectomy procedures are
- laminotomy and discectomy
- microdiscectomy
Laminotomy and Discectomy
Laminotomy and discectomy is the traditional method of removing the disc. Laminotomy is taking off part of the lamina bone (the back of the ring over the spinal canal). This allows greater room for the surgeon to take out part of the disc (discectomy).
An incision is made down the middle of the low back. After separating the tissues to expose the bones along the low back, the surgeon takes an X-ray to make sure that the procedure is being performed on the correct disc. A cutting tool is used to remove a small section of the lamina bone.
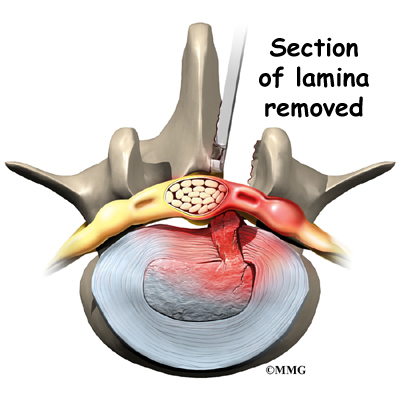
Next, the surgeon cuts a small opening in the ligamentum flavum, the long ligament between the lamina and the spinal cord. This exposes the nerves inside the spinal canal. The painful nerve root is gently moved aside so the injured disc can be examined. A hole is cut in the outside rim of the disc. Forceps are placed inside the hole in order to clean out disc material within the disc. Then the surgeon carefully looks inside and outside the disc space to locate and remove any additional disc fragments.
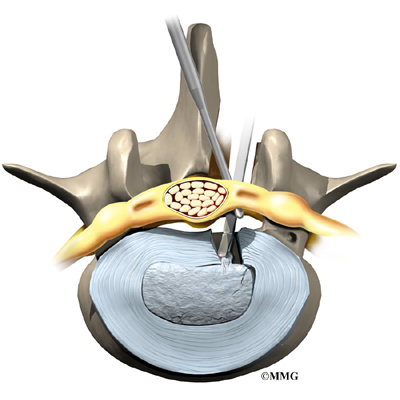
Finally, the nerve root is checked for tension. If it doesn’t move freely, the surgeon may cut a larger opening in the neural foramen, the nerve passage between the vertebrae.
Before closing and suturing the wound, some surgeons will implant a special foam pad or a piece of fat over the nerve root to keep scar tissue from growing onto the nerve. Some surgeons also insert a small drain tube in the wound.
Microdiscectomy
The surgeon performs microdiscectomy using a surgical microscope. A two-inch incision is made in the low back directly over the problem disc. The skin and soft tissues are separated to expose the bones along the back of the spine. An X-ray of the low back is taken to ensure the surgeon works on the right disc.
A retractor is used to spread apart the lamina bones above and below the disc. Then the surgeon makes a tiny slit in the ligamentum flavum, exposing the spinal nerves. A special hook is placed under the spinal nerve root. The hook is used to lift the nerve root, so the surgeon can see the injured disc.
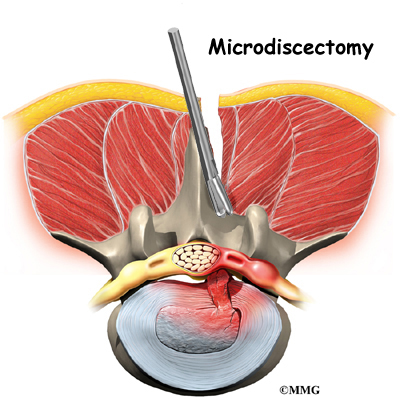
Next, the annulus (outer ring) of the disc is sliced open. Material from inside the disc is scooped out to ensure the disc doesn’t herniate again. Since only the injured portion is removed, the disc is left intact and functioning. Then the surgeon inspects the area around the nerve root and removes any loose disc fragments. Finally, the nerve root is gently wiggled to make sure it is free to move. If it can’t move, the surgeon also cleans around the neural foramen, the nerve passage between the two vertebrae. When the nerve moves freely, the muscles and soft tissues are put back in place, and the skin is stitched together.
Complications
What might go wrong?
As with all major surgical procedures, complications can occur. Some of the most common complications following lumbar discectomy include
- problems with anesthesia
- thrombophlebitis
- infection
- nerve damage
- ongoing pain
This is not intended to be a complete list of possible complications.
Problems with Anesthesia
Problems can arise when the anesthesia given during surgery causes a reaction with other drugs the patient is taking. In rare cases, a patient may have problems with the anesthesia itself. In addition, anesthesia can affect lung function because the lungs don’t expand as well while a person is under anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Thrombophlebitis (Blood Clots)
View animation of pulmonary embolism
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can occur after any operation. It occurs when the blood in the large veins of the leg forms blood clots. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lung, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Most surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective is getting you moving as soon as possible. Two other commonly used preventative measures include
- pressure stockings to keep the blood in the legs moving
- medications that thin the blood and prevent blood clots from forming
Infection
Infection following spine surgery is rare but can be a very serious complication. Some infections may show up early, even before you leave the hospital. Infections on the skin’s surface usually go away with antibiotics. Deeper infections that spread into the bones and soft tissues of the spine are harder to treat. They may require additional surgery to treat the infected portion of the spine.
Nerve Damage
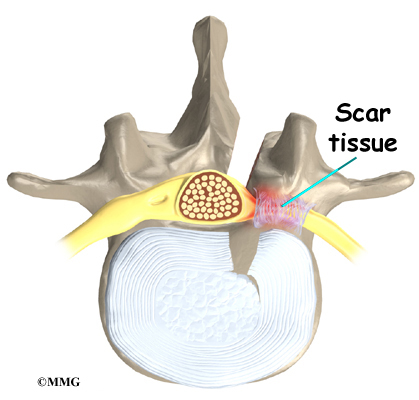
Any surgery that is done near the spinal canal can potentially cause injury to the spinal cord or spinal nerves. Injury can occur from bumping or cutting the nerve tissue with a surgical instrument, from swelling around the nerve, or from the formation of scar tissue. An injury to the spinal cord or spinal nerves can cause muscle weakness and a loss of sensation to the areas supplied by the nerve.
Ongoing Pain
Discectomy is especially helpful for patients whose main complaint before surgery is leg pain. When back pain has been the main complaint, however, surgical results vary. If the pain continues after surgery or becomes unbearable, talk to your surgeon about treatments that can help control your pain.
After Surgery
What happens after surgery?
Patients are usually able to get out of bed within a few hours after surgery. However, you will be instructed to move your back only carefully and comfortably. The drain tube is normally taken out the day after surgery. Patients are able to return home when their medical condition is stable.
Most patients leave the hospital the day after surgery. They are usually safe to drive within a week or two. Bending and lifting should be avoided for four to six weeks. People generally get back to light work in two to four weeks and can do heavier work and sports within two to three months. Workers whose jobs involve strenuous manual labor may be counseled to consider a less strenuous job.
Patients usually begin outpatient physical therapy two to three weeks after the date of surgery.
Rehabilitation
What should I expect as I recover?
Many surgeons prescribe outpatient physical therapy within three weeks after surgery. Physical therapy after lumbar discectomy is generally only needed for six to eight weeks. You should expect full recovery to take up to four months.
At first, therapy focuses on controlling pain and inflammation. Ice and electrical stimulation treatments are commonly used to help with these goals. Your therapist may also use massage and other hands-on techniques to ease muscle spasm and pain.
Active treatments are added slowly. These include exercises for improving heart and lung function. Walking and swimming are ideal cardiovascular exercises after this type of surgery. Therapists also teach specific exercises to help tone and control the muscles that stabilize the low back.
Your therapist works with you on how to move and do activities. This form of treatment, called body mechanics, helps you develop new movement habits. This training helps you keep your back in safe positions as you go about your work and daily activities. At first, this may be as simple as learning how to move safely and easily in and out of bed, how to get dressed and undressed, and how to do some of your routine activities. Then you learn how to keep your back safe while you lift and carry items and as you begin to do more strenuous activities.
As your condition improves, your therapist tailors your program to help prepare you to go back to work. Some patients are not able to go back to a previous job that requires strenuous tasks. However, your therapist may suggest changes in job tasks that enable you to go back to your previous job. Your therapist may also suggest alternate forms of work. You’ll learn to do your tasks in ways that keep your back safe and free of extra strain.
Before your therapy sessions end, your therapist will teach you a number of ways to avoid future problems.
Low Back Pain
A Patient’s Guide to Low Back Pain
Introduction
Low back pain is one of the main reasons Americans visit their doctor. For adults over 40, it ranks third as a cause for doctor visits, after heart disease and arthritis.
Eighty percent of people will have low back pain at some point in their lives. And nearly everyone who has low back pain once will have it again.
Very few people who feel pain in their low back have a serious medical problem. Ninety percent of people who experience low back pain for the first time get better in two to six weeks. Only rarely do people with low back pain develop chronic back problems.
With these facts in mind, you can be assured that back pain is common, that it usually only causes problems for a short period of time, and that you can take steps to ease symptoms and prevent future problems.
This guide will help you understand
- which parts make up the spine and low back
- what causes low back pain, and what the most common symptoms are
- what tests your doctor may run
- how to manage your pain and prevent future problems
Anatomy
Which parts make up the lumbar spine, and how do they work?
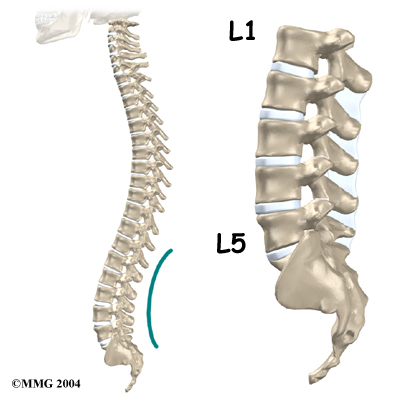
The human spine is made up of 24 spinal bones, called vertebrae Vertebrae are stacked on top of one another to create the spinal column. The spinal column gives the body its form. It is the body’s main upright support.
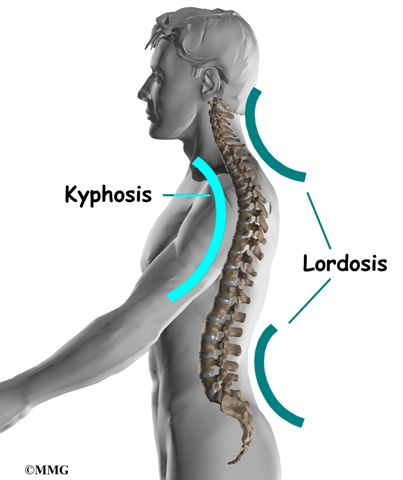
From the side, the spine forms three curves. The neck, called the cervical spine, curves slightly inward. The mid back, or thoracic spine curves outward. The outward curve of the thoracic spine is called kyphosis. The low back, also called the lumbar spine, curves slightly inward. An inward curve of the spine is called lordosis.
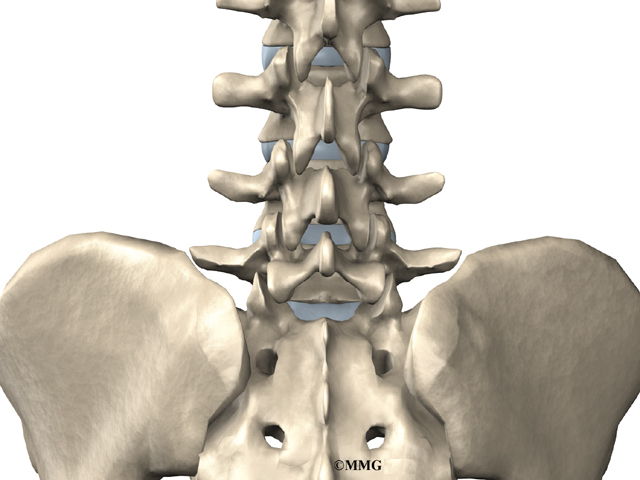
The lumbar spine is made up of the lower five vertebrae. Doctors often refer to these vertebrae as L1 to L5. The lowest vertebra of the lumbar spine, L5, connects to the top of the sacrum, a triangular bone at the base of the spine that fits between the two pelvic bones. Some people have an extra, or sixth, lumbar vertebra. This condition doesn’t usually cause any particular problems.
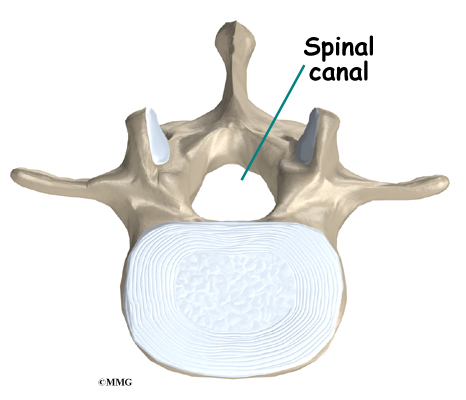
Each vertebra is formed by a round block of bone, called a vertebral body. The lumbar vertebral bodies are taller and bulkier compared to the rest of the spine. This is partly because the low back has to withstand pressure from body weight and from daily actions like lifting, carrying, and twisting. Also, large and powerful muscles attaching on or near the lumbar spine place extra force on the lumbar vertebral bodies.
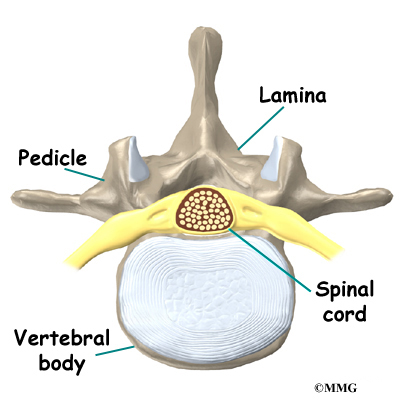
A bony ring attaches to the back of each vertebral body. When the vertebrae are stacked on top of each other, these rings form a hollow tube. This bony tube surrounds the spinal cord as it passes through the spine. Just as the skull protects the brain, the bones of the spinal column protect the spinal cord.
The spinal cord extends down to the L2 vertebra. Below this level, the spinal canal encloses a bundle of nerves that goes to the lower limbs and pelvic organs.

The Latin term for this bundle of nerves is cauda equina, meaning horse’s tail.
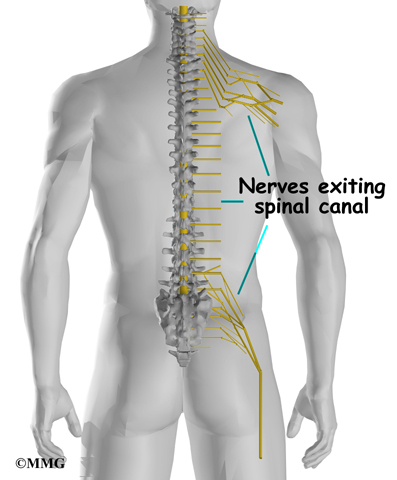
As the spinal cord travels from the brain down through the spine, it sends out nerves on the sides of each vertebra called nerve roots. These nerve roots join together to form the nerves that travel throughout the body and form the body’s electrical system. The nerve roots that come out of the lumbar spine form the nerves that go to the lower limbs and pelvis. The thoracic spine nerves go to the abdomen and chest. The nerves coming out of the cervical spine go to the neck, shoulders, arms, and hands.

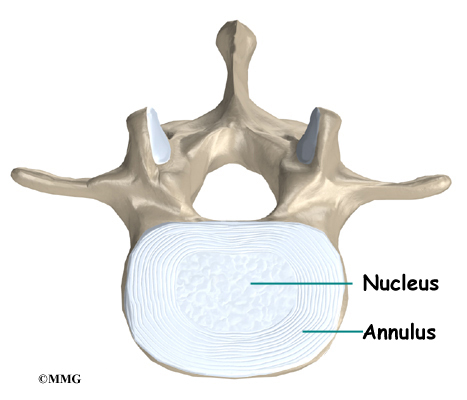
It is sometimes easier to understand what happens in the spine by looking at a spinal segment. A spinal segment includes two vertebrae separated by an intervertebral disc, the nerves that leave the spinal cord at that level, and the small facet joints that link each level of the spinal column.
The intervertebral disc normally works like a shock absorber. It protects the spine against the daily pull of gravity. It also protects the spine during heavy activities that put strong force on the spine, such as jumping, running, and lifting.
An intervertebral disc is made up of two parts. The center, called the nucleus, is spongy. It provides most of the disc’s ability to absorb shock. The nucleus is held in place by the annulus, a series of strong ligament rings surrounding it. Ligaments are strong connective tissues that attach bones to other bones.
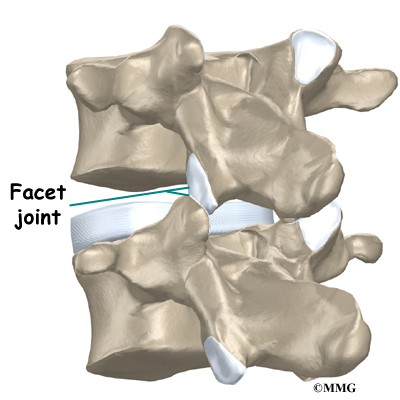
Between the vertebrae of each spinal segment are two facet joints. The facet joints are located on the back of the spinal column. There are two facet joints between each pair of vertebrae, one on each side of the spine. A facet joint is made of small, bony knobs that line up along the back of the spine. Where these knobs meet, they form a joint that connects the two vertebrae. The alignment of the facet joints of the lumbar spine allows freedom of movement as you bend forward and back.
The surfaces of the facet joints are covered by articular cartilage. Articular cartilage is a smooth, rubbery material that covers the ends of most joints. It allows the bone ends to move against each other smoothly, without pain.
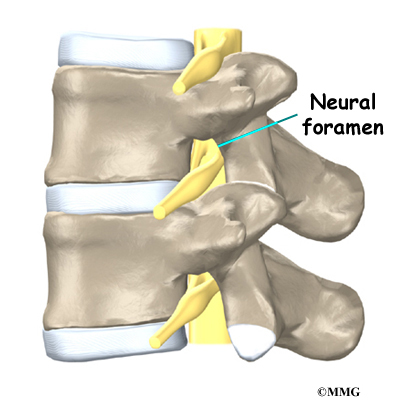
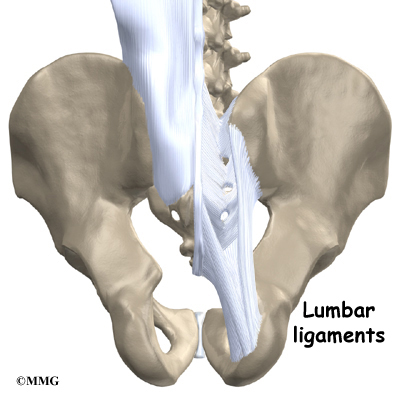
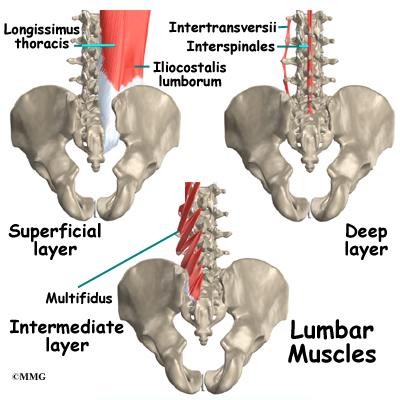
Two spinal nerves exit the sides of each spinal segment, one on the left and one on the right. As the nerves leave the spinal cord, they pass through a small bony tunnel on each side of the vertebra, called a neural foramen. (The term used to describe more than one opening is neural foramina.)
The lumbar spine is supported by ligaments and muscles. The ligaments are arranged in various layers and run in multiple directions. Thick ligaments connect the bones of the lumbar spine to the sacrum (the bone below L5) and pelvis.
The muscles of the low back are also arranged in layers. Those closest to the surface are covered by a thick tissue called fascia.
The middle layer, called the erector spinae, has strap-shaped muscles that run up and down over the lower ribs, chest, and low back. They blend in the lumbar spine to form a thick tendon that binds the bones of the low back, pelvis, and sacrum.
The deepest layer of muscles connects along the back surface of the spine bones. The muscles also connect the low back, pelvis, and sacrum. These deepest muscles coordinate their actions with the muscles of the abdomen to help hold the spine steady during activity.
Causes
Why do I have low back pain?
There are many causes of low back pain. Doctors are not always able to pinpoint the source of a patient’s pain. But your doctor will make every effort to ensure that your symptoms are not from a serious medical cause, such as cancer or a spinal infection.
The vast majority of back problems are a result of wear and tear on the parts of the spine over many years. This process is called degeneration. Over time, the normal process of aging can result in degenerative changes in all parts of the spine.
Injuries to the spine, such as a fracture or injury to the disc, can make the changes happen even faster. There is strong evidence that cigarette smoking also speeds up degeneration of the spine. Scientists have found links among family members, showing that genetics plays a role in how fast these changes occur.
Degeneration
The intervertebral disc changes over time. At first, the disc is spongy and firm. The nucleus in the center of the disc contains a great deal of water. This gives the disc its ability to absorb shock and protect the spine from heavy and repeated forces.
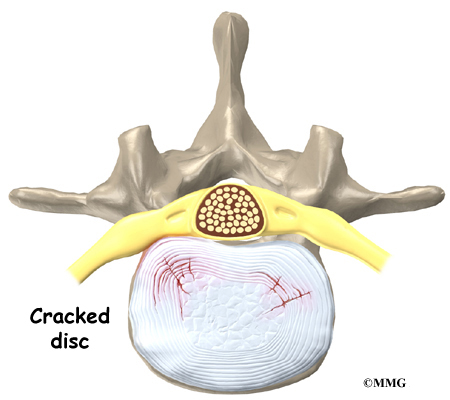
The first change that occurs is that the annulus around the nucleus weakens and begins to develop small cracks and tears. The body tries to heal the cracks with scar tissue. But scar tissue is not as strong as the tissue it replaces. The torn annulus can be a source of pain for two reasons. First, there are pain sensors in the outer rim of the annulus. They signal a painful response when the tear reaches the outer edge of the annulus. Second, like injuries to other tissues in the body, a tear in the annulus can cause pain due to inflammation.
With time, the disc begins to lose water, causing it to lose some of its fullness and height. As a result, the vertebrae begin to move closer together.

As the disc continues to degenerate, the space between the vertebrae shrinks. This compresses the facet joints along the back of the spinal column. As these joints are forced together, extra pressure builds on the articular cartilage on the surface of the facet joints. This extra pressure can damage the facet joints. Over time, this may lead to arthritis in the facet joints.
These degenerative changes in the disc, facet joints, and ligaments cause the spinal segment to become loose and unstable. The extra movement causes even more wear and tear on the spine. As a result, more and larger tears occur in the annulus.
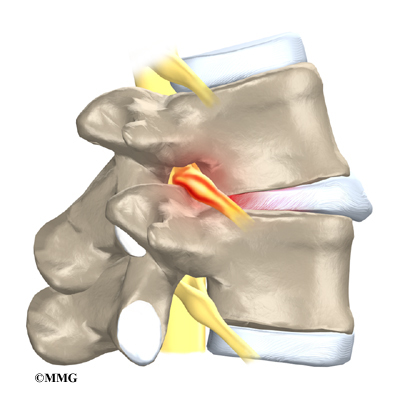
The nucleus may push through the torn annulus and into the spinal canal. This is called a herniated or ruptured disc. The disc material that squeezes out can press against the spinal nerves. The disc also emits enzymes and chemicals that produce inflammation. The combination of pressure on the nerves and inflammation caused by the chemicals released from the disc cause pain.
View animation of degeneration
As the degeneration continues, bone spurs develop around the facet joints and around the disc. No one knows exactly why these bone spurs develop. Most doctors think that bone spurs are the body’s attempt to stop the extra motion between the spinal segment. These bone spurs can cause problems by pressing on the nerves of the spine where they pass through the neural foramina. This pressure around the irritated nerve roots can cause pain, numbness, and weakness in the low back, buttocks, and lower limbs and feet.
A collapsed spinal segment eventually becomes stiff and immobile. Thickened ligaments and facet joints, scarred and dried disc tissue, and protruding bone spurs prevent normal movement. Typically, a stiff joint doesn’t cause as much pain as one that slides around too much. So this stage of degeneration may actually lead to pain relief for some people.
Mechanical and Neurogenic Pain
To best understand the cause of your pain, spine specialists sometimes divide low back pain into two categories:
- mechanical pain
- neurogenic pain
Mechanical Pain

Mechanical back pain is caused by wear and tear in the parts of the lumbar spine. This type of pain is similar in nature to a machine that begins to wear out. Mechanical pain usually starts from degenerative changes in the disc. As the disc begins to collapse and the space between the vertebrae narrows, the facet joints may become inflamed. Mechanical pain typically gets worse after activity due to strain on the moving parts of the spine. Mechanical pain is usually felt in the back, but it may spread into the buttocks, hips, and thighs. The pain rarely goes down past the knee. Mechanical back pain usually doesn’t cause weakness or numbness in the leg or foot, because the problem is not from pressure on the spinal nerves.
Neurogenic Pain
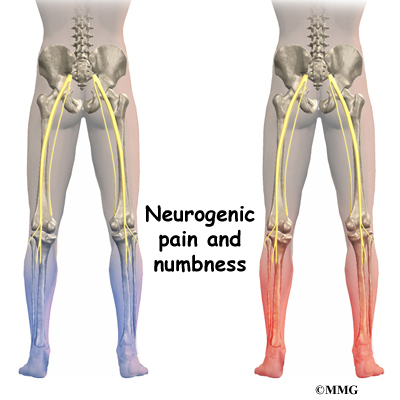
Neurogenic pain means pain from nerve injury. Neurogenic pain occurs when spinal nerves are inflamed, squeezed, or pinched. This can happen when a disc herniates or when a nerve gets pinched where it leaves the spine. Recently it has also become known that when a disc ruptures, chemicals are released that inflame the nerves even if there is no pressure directly on the nerve. Neurogenic symptoms concern doctors more than mechanical pain because they can signal damage to the nerves and lead to weakness or numbness in the lower extremities.
The nerve pressure causes symptoms in the areas where the nerve travels, rather than in the low back. This happens because pressure on the spinal nerve affects structures away from the spine, such as the muscles. As a result, a person’s back may not hurt, yet the person feels pain, numbness, or weakness in the leg or foot. This indicates there’s a problem with the body’s electrical wiring. The pressure on the nerve affects how the body functions. Muscles weaken. Reflexes slow. Sensations of pins, needles, and numbness may be felt where the nerve travels.
Spine Conditions
The effects of spine degeneration or back injury can lead to specific spine conditions. These include
- annular tears
- internal disc disruption
- herniated disc
- facet joint arthritis
- segmental instability
- spinal stenosis
- foraminal stenosis
Annular Tears
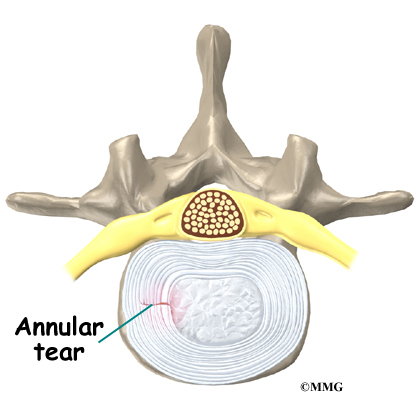
Our intervertebral discs change with age, much like our hair turns gray. Perhaps the earliest stage of degeneration occurs due to tears that occur in the annulus. These tears can result from wear and tear over a period of time. They can also be the result of a sudden injury to the disc due to a twist or increased strain on the disc that overpowers the strength of the annulus. These annular tears may cause pain in the back until they heal with scar tissue.
View animation of annular tearing
Related Document: A Patient’s Guide to Lumbar Degenerative Disc Disease
Internal Disc Disruption
Multiple annular tears can lead to a disc that becomes weak. The disc starts to degenerate and collapse. The vertebrae begin to compress together. The collapsing disc can be the source of pain because it has lost the ability to be a shock absorber between the vertebrae. This condition is sometimes referred to as internal disc disruption. This type of problem causes primarily mechanical back pain due to inflammation of the disc and surrounding structures.
Herniated Disc
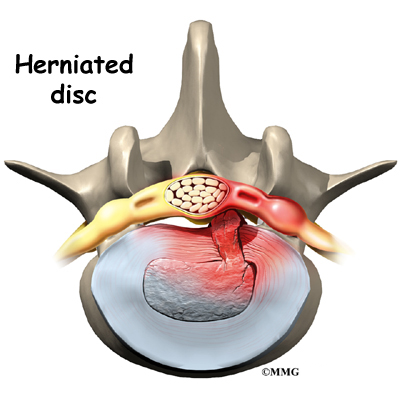
A disc that has been weakened may rupture or herniate. If the annulus ruptures, or tears, the material in the nucleus can squeeze out of the disc, or herniate. A disc herniation usually causes compressive problems if the disc presses against a spinal nerve. The chemicals released by the disc may also inflame the nerve root, causing pain in the area where the nerve travels down the leg. This type of pain is referred to as sciatica.
Even a normal disc can rupture. Heavy, repetitive bending, twisting, and lifting can place too much pressure on the disc, causing the annulus to tear and the nucleus to rupture into the spinal canal.
Related Document: A Patient’s Guide to Lumbar Disc Herniation
Facet Joint Arthritis
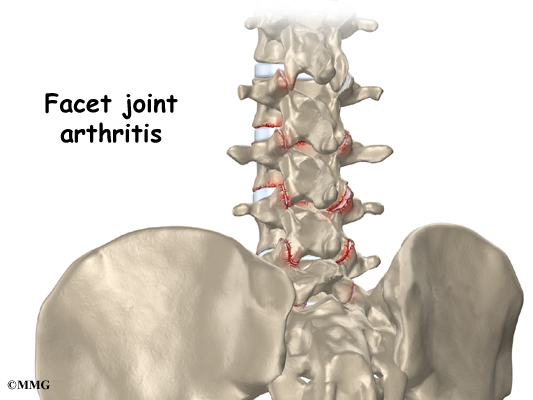
The facet joints along the back of the spinal column link the vertebrae together. They are not meant to bear much weight. However, if a disc loses its height, the vertebra above the disc begins to compress toward the one below. This causes the facet joints to press together. Articular cartilage covers the surfaces where these joints meet. Like other joints in the body that are covered with articular cartilage, the facet joints can develop osteoarthritis as the articular cartilage wears away over time. Extra pressure on the facet joints, such as that from a collapsing disc, can speed the degeneration in the facet joints. The swelling and inflammation from an arthritic facet joint can be a source of low back pain.
Related Document: A Patient’s Guide to Lumbar Facet Joint Arthritis
Segmental Instability

Segmental instability means that the vertebral bones within a spinal segment move more than they should. In the lumbar spine, this can develop if the disc has degenerated. Usually the supporting ligaments around the vertebrae have also been stretched over time.
Segmental instability also includes conditions in which a vertebral body begins to slip over the one below it. When a vertebral body slips too far forward, the condition is called spondylolisthesis. Whatever the cause, this extra movement in the bones of the spine can create problems. It can lead to mechanical pain simply because the structures of the spine move around too much and become inflamed and painful. The extra movement can also cause neurogenic symptoms if the spinal nerves are squeezed as a result of the segmental instability.
Related Document: A Patient’s Guide to Lumbar Spondylolisthesis
Spinal Stenosis
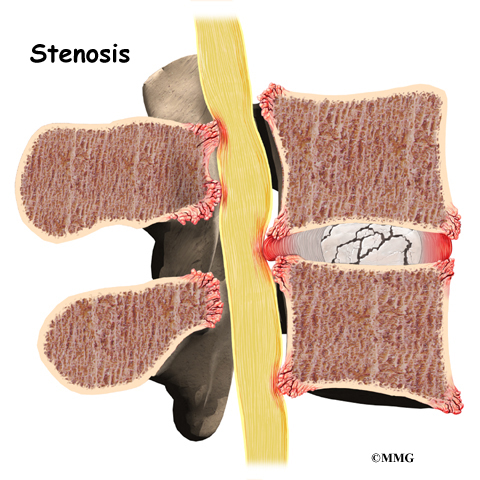
Stenosis means closing in. Spinal stenosis refers to a condition in which the tissues inside the spinal canal are closed in, or compressed. The spinal cord ends at L2. Below this level, the spinal canal contains only spinal nerves that travel to the pelvis and legs. When stenosis narrows the spinal canal, the spinal nerves are squeezed inside the canal.
The pressure from the condition can cause problems in the way the nerves work. The resulting problems include pain and numbness in the buttocks and legs and weakness in the muscles supplied by the nerves. Because these nerves travel to the bladder and rectum, weakness in the these muscles can cause problems with control of the bladder and bowels.
Related Document: A Patient’s Guide to Lumbar Spinal Stenosis
Foraminal Stenosis
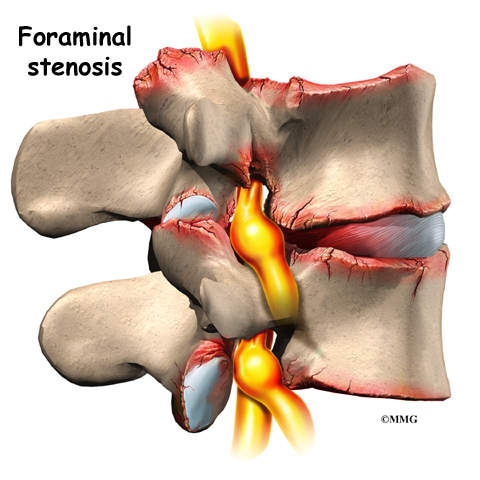
Spinal nerves exit the spinal canal between the vertebrae in a tunnel called the neural foramen. Anything that causes this tunnel to become smaller can squeeze the spinal nerve where it passes through the tunnel. This condition is called foraminal stenosis, meaning the foramen is narrowed. As the disc collapses and loses height, the vertebral body above begins to collapse toward the one below. The opening around the nerve root narrows, squeezing the nerve. Arthritis of the facet joints causes bone spurs to form and point into the foramen, causing further nerve compression and irritation. Foraminal stenosis can cause a combination of mechanical pain and neurogenic pain from the irritated nerve root.
Related Document: A Patient’s Guide to Lumbar Disc Herniation
Symptoms
What are some of the symptoms of low back problems?
Symptoms from low back problems vary. They depend on a person’s condition and which structures are affected. Some of the more common symptoms of low back problems are
- low back pain
- pain spreading into the buttocks and thighs
- pain radiating from the buttock to the foot
- back stiffness and reduced range of motion
- muscle weakness in the hip, thigh, leg, or foot
- sensory changes (numbness, prickling, or tingling) in the leg, foot, or toes
Rarely, symptoms involve changes in bowel or bladder function. A large disc herniation that pushes straight back into the spinal canal can put pressure on the nerves that go to the bowels and bladder. The pressure may cause symptoms of low back pain, pain running down the back of both legs, and numbness or tingling between the legs in the area you would contact if you were seated on a saddle. The pressure on the nerves can cause a loss of control in the bowels or bladder.
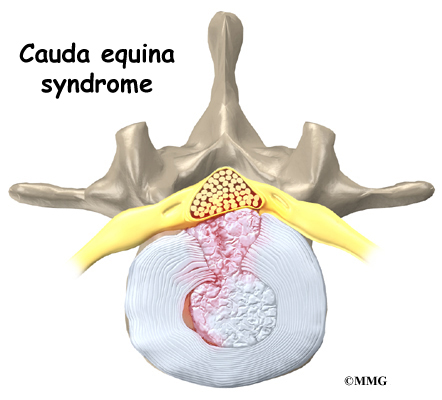
This is an emergency.
If the pressure isn’t relieved, it can lead to permanent paralysis of the bowels and bladder. This condition is called cauda equina syndrome. Doctors recommend immediate surgery to remove pressure from the nerves.
Diagnosis
How will my doctor find out what’s causing my problem?
The diagnosis of low back problems begins with a thorough history of your condition. You might be asked to fill out a questionnaire describing your back problems. Your doctor will ask you questions to find out when you first started having problems, what makes your symptoms worse or better, and how the symptoms affect your daily activity. Your answers will help guide the physical examination.
Your doctor will then physically examine the muscles and joints of your low back. It is important that your doctor see how your back is aligned, how it moves, and exactly where it hurts.
Your doctor may do some simple tests to check the function of the nerves. These tests are used to measure the strength in your lower limbs, check your reflexes, and determine whether you have numbness in your legs or feet.
The information from your medical history and physical examination will help your doctor decide which further tests to run. The tests give different types of information.
Radiological Imaging
Radiological imaging tests help your doctor see the anatomy of your spine. There are several kinds of imaging tests that are commonly used.
X-rays
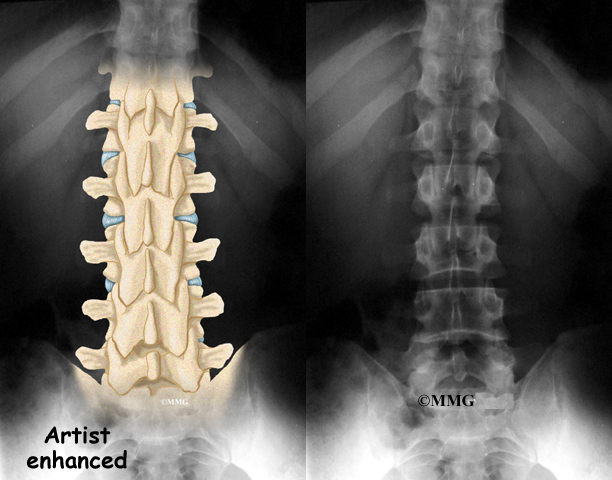
X-rays show problems with bones, such as infection, bone tumors, or fractures. X-rays of the spine also can give your doctor information about how much degeneration has occurred in the spine, such as the amount of space in the neural foramina and between the discs. X-rays are usually the first test ordered before any of the more specialized tests.
Flexion and Extension X-rays
Special X-rays called flexion and extension X-rays may help to determine if there is instability between vertebrae. These X-rays are taken from the side as you lean as far forward and then as far backward as you can. Comparing the two X-rays allows the doctor to see how much motion occurs between each spinal segment.
MRI Scans

The magnetic resonance imaging (MRI) scan uses magnetic waves to create pictures of the lumbar spine in slices. The MRI scan shows the lumbar spine bones as well as the soft tissue structures such as the discs, joints, and nerves. MRI scans are painless and don’t require needles or dye. The MRI scan has become the most common test to look at the lumbar spine after X-rays have been taken.
CT Scans
The computed tomography (CT) scan is a special type of X-ray that lets doctors see slices of bone tissue. The machine uses a computer and X-rays to create these slices. It is used primarily when problems are suspected in the bones.
Myelogram
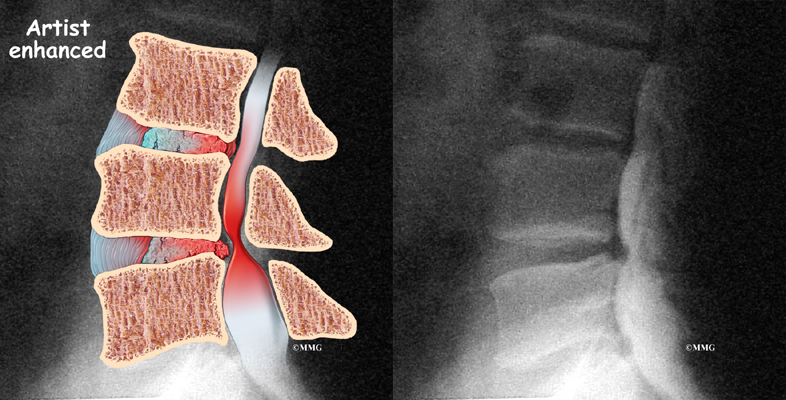
The myelogram is a special kind of X-ray test where a special dye is injected into the spinal sac. The dye shows up on an X-ray. It helps a doctor see if there is a herniated disc, pressure on the spinal cord or spinal nerves, or a spinal tumor. Before the CT scan and the MRI scan were developed, the myelogram was the only test that surgeons had to look for a herniated disc. The myelogram is still used today but not nearly as often. The myelogram is usually combined with CT scan to give more detail.
Discogram
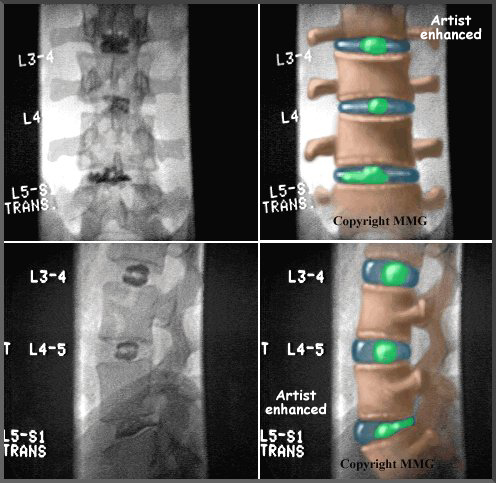
The discogram is another specialized X-ray test. A discogram has two parts. First, a needle is inserted into the problem disc, and saline is injected into the disc to create pressure inside the disc. If this reproduces your pain, then it suggests that the disc is the source of your pain. During the second part of the test, dye is injected into the disc. The dye can be seen on X-ray. Using both regular X-rays and CT scan images, the dye outlines the inside of the disc. This can show abnormalities of the nucleus such as annular tears and ruptures of the disc.
Bone Scan
A bone scan is a special test where radioactive tracers are injected into your blood stream. The tracers then show up on special X-rays of your back. The tracers build up in areas where bone is undergoing a rapid repair process, such as a healing fracture or the area surrounding an infection or tumor. Usually the bone scan is used to locate the problem. Other tests such as the CT scan or MRI scan are then used to look at the area in detail.
Other Tests
Your doctor may also ask you to do other tests.
Electromyogram
An electromyogram (EMG) is a special test used to determine if there are problems with any of the nerves going to the lower limbs. EMGs are usually done to determine whether the nerve roots have been pinched by a herniated disc. During the test, small needles are placed into certain muscles that are supplied by each nerve root. If there has been a change in the function of the nerve, the muscle will send off different types of electrical signals. The EMG test reads these signals and can help determine which nerve root is involved.
Laboratory Tests
Not all causes of low back pain are from degenerative conditions. Doctors use blood tests to identify other conditions, such as arthritis or infection. Low back pain can be caused by problems that do not involve the spine, such as stomach ulcers, kidney problems, and aneurysms of the aorta. Other tests may be needed to rule out problems that do not involve the spine.
Treatment
What can be done to relieve my symptoms?
Ninety percent of people who experience low back pain for the first time get better in two to six weeks without any treatment at all. Patients often do best when encouraged to stay active and to get back to normal activities as soon as possible, even if there is still some pain. The pain may not go away completely. One goal of treatment is to help you find ways to control the pain and allow you to continue to do your normal activities.
Nonsurgical Treatment
Whenever possible, doctors prefer to use treatments other than surgery. The first goal of these nonsurgical treatments is to ease your pain and other symptoms.
Bed Rest
In cases of severe pain, doctors may suggest a short period of bed rest, usually no more than two days. Lying on your back can take pressure off sore discs and nerves. Most doctors advise against strict bed rest and prefer that patients do ordinary activities using pain to gauge how much is too much.

Back Brace
A back support belt is sometimes recommended when back pain first strikes. It can help provide support and lower the pressure inside a problem disc. Patients are encouraged to gradually discontinue wearing the support belt over a period of two to four days. Otherwise, back muscles begin to rely on the belt and start to shrink (atrophy).
Medications
Many different types of medications are typically prescribed to help gain control of the symptoms of low back pain. There is no medication that will cure low back pain. Medications are prescribed to help with sleep disturbances and to help control pain, inflammation, and muscle spasm.
Physical Therapy and Exercise
In addition to other nonsurgical treatments, doctors often ask their patients to work with a physical therapist. Therapy treatments focus on relieving pain, improving back movement, and fostering healthy posture. A therapist can design a rehabilitation program to address a particular condition and to help the patient prevent future problems. There is a great deal of scientific proof that exercise and increased overall fitness reduce the risk of developing back pain and can improve the symptoms of back pain once it begins.
Injections
Spinal injections are used for both treatment and diagnostic purposes. There are several different types of spinal injections that your doctor may suggest. These injections usually use a mixture of an anesthetic and some type of cortisone preparation. The anesthetic is a medication that numbs the area where it is injected. If the injection takes away your pain immediately, this gives your doctor important information suggesting that the injected area is indeed the source of your pain. The cortisone decreases inflammation and can reduce the pain from an inflamed nerve or joint for a prolonged period of time.
Some injections are more difficult to perform and require the use of a fluoroscope. A fluoroscope is a special type of X-ray that allows the doctor to see an X-ray picture continuously on a TV screen. The fluoroscope is used to guide the needle into the correct place before the injection is given.
- Epidural Steroid Injection (ESI): Back pain from inflamed nerve roots and facet joints may benefit from an epidural steroid injection (ESI). In an ESI, the medication mixture is injected into the epidural space around the nerve roots. Generally, an ESI is given only when other nonoperative treatments aren’t working. ESIs are not always successful in relieving pain. If they do work, they may only provide temporary relief.
- Selective Nerve Root Injection: Another type of injection to place steroid medication around a specific inflamed nerve root is called a selective nerve root injection. The fluoroscope is used to guide a needle directly to the painful spinal nerve root. The nerve root is then bathed with the medication. Some doctors believe this procedure gets more medication to the painful spot. In difficult cases, the selective nerve root injection can also help surgeons decide which nerve root is causing the problem before surgery is planned.
- Facet Joint Injection: When the problem is thought to be in the facet joints, an injection into one or more facet joints can help determine which joints are causing the problem and ease the pain as well. The fluoroscope is used to guide a needle directly into the facet joint. The facet joint is then filled with medication mixture. If the injection immediately eases the pain, it helps confirm that the facet joint is a source of pain. The steroid medication will reduce the inflammation in the joint over a period of days and may reduce or eliminate your back pain.
 Trigger Point Injections: Injections of anesthetic medications mixed with a cortisone medication are sometimes given in the muscles, ligaments, or other soft tissues near the spine. These injections are called trigger point injections. These injections can help relieve back pain and ease muscle spasm and tender points in the back muscles.
Trigger Point Injections: Injections of anesthetic medications mixed with a cortisone medication are sometimes given in the muscles, ligaments, or other soft tissues near the spine. These injections are called trigger point injections. These injections can help relieve back pain and ease muscle spasm and tender points in the back muscles.
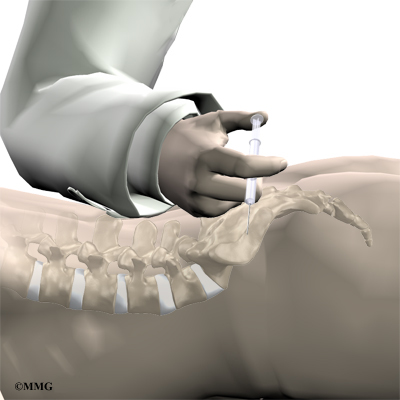
Surgery
Only rarely is lumbar spine surgery scheduled right away. Your doctor may suggest immediate surgery if you are losing control of your bowels and bladder or if your muscles are becoming weaker very rapidly.
For other conditions, doctors prefer to try nonsurgical treatments for a minimum of three months before considering surgery. Most people with back pain tend to get better, not worse. Even people who have degenerative spine changes tend to gradually improve with time. Only one to three percent of patients with degenerative lumbar conditions typically require surgery. Surgery may be suggested when severe pain is not improving.
There are many different operations for back pain. The goal of nearly all spine operations is to remove pressure from the nerves of the spine, stop excessive motion between two or more vertebrae, or both. The type of surgery that is best depends on that patient’s conditions and symptoms.
Laminectomy
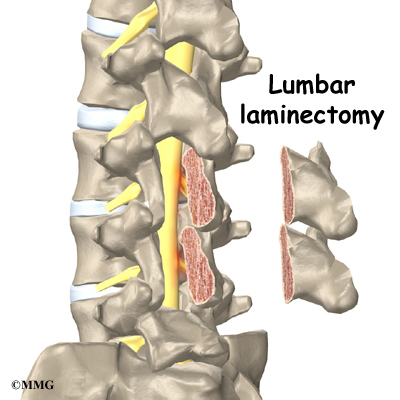
The lamina is the covering layer of the bony ring of the spinal canal. It forms a roof-like structure over the back of the spinal column. When the nerves in the spinal canal are being squeezed by a herniated disc or from bone spurs pushing into the canal, a laminectomy removes part or all of the lamina to release pressure on the spinal nerves.
Related Document: A Patient’s Guide to Lumbar Laminectomy
Discectomy
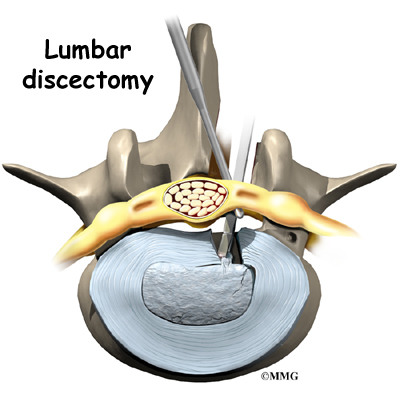
When the intervertebral disc has ruptured, the portion that has ruptured into the spinal canal may put pressure on the nerve roots. This may cause pain, weakness, and numbness that radiates into one or both legs. The operation to remove the portion of the disc that is pressing on the nerve roots is called a discectomy. This operation is performed through an incision in the low back immediately over the disc that has ruptured.
Many spine surgeons now perform discectomy procedures that require only small incisions in the low back (minimally invasive). The advantage of these minimally invasive procedures is less damage to the muscles of the back and a quicker recovery. Many surgeons are now performing minimally invasive discectomy as an outpatient procedure.
Related Document: A Patient’s Guide to Lumbar Discectomy
Lumbar Fusion
When there is excessive motion between two or more vertebrae, the excess motion can cause both mechanical pain and irritation of the nerves of the lumbar spine. In this case some type of spinal fusion is usually recommended. The goal of a spinal fusion is to force two or more vertebrae to grow together, or fuse, into one bone. A solid fusion between two vertebrae stops the movement between the two bones. The pain is reduced because the fusion reduces the constant irritation and inflammation of the nerve roots. There are many different types of spinal fusions.
- Posterior Lumbar Fusion: In the past, the traditional operation to perform a fusion of the lumbar spine was to decorticate the back surface of the vertebrae. Decorticate means to remove the hard outside covering of a bone to create a bleeding bone surface. Once this was done, bone graft was taken from the pelvis and laid on top of the decorticated vertebrae. The body tries to heal this area just like it would a fractured bone. The bone graft and the bleeding bone grow together and fuse to create one solid bone. Spinal fusions were not always successful, mainly because the vertebrae failed to fuse together in up to 20 percent of cases. Surgeons began looking for ways to increase the success of fusions. For many years, metal plates and screws have been used to treat fractures of other bones. The more rigid two bones can be held together while the healing phase occurs, the more likely the bones are to heal. Spine surgeons began looking for ways to hold the vertebrae together while the fusion took place.
Related Document: A Patient’s Guide to Posterior Lumbar Fusion
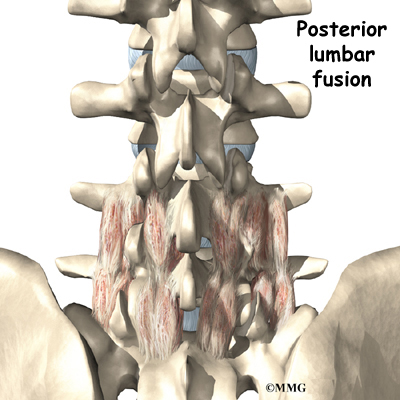
- Posterior Lumbar Instrumented Fusion: Major advances have been made in recent years in developing metal rods, metal plates, and special screws that are designed to hold the vertebrae together while the fusion takes place. These new techniques of spinal fusion are referred to as instrumented fusions because of the special devices used to secure the vertebrae to be fused. Today the most common type of posterior fusion is performed using special screws called pedicle screws that are inserted into each vertebra and connected to either a metal plate or metal rod along the back of the spine. The vertebrae are still decorticated, and bone graft is still used to stimulate the bones to heal together and fuse into one solid bone.
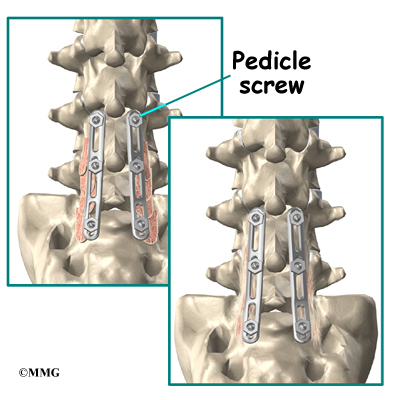
- Anterior Lumbar Interbody Fusion: A fusion of the lumbar spine can be accomplished in other ways. In some cases, surgeons feel that it is best to perform a fusion from the front of the spine. This is termed an anterior interbody fusion. This type of fusion requires an incision in the side of the abdomen to allow the surgeon to see the front of the spine. The intervertebral disc is removed between two vertebral bodies and bone graft is inserted where the disc was removed. The two vertebral bodies heal together and fuse.Related Document: A Patient’s Guide to Anterior Lumbar Interbody Fusion
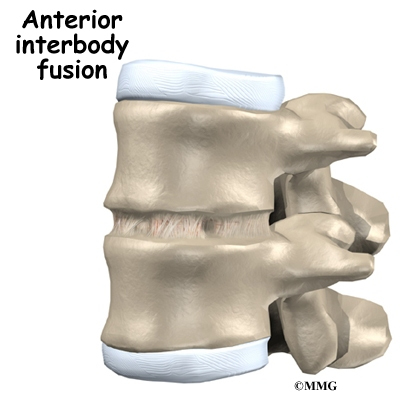
- Anterior Lumbar Discectomy and Fusion with Cages: Degeneration of the intervertebral disc allows the vertebrae to move closer together, which narrows the openings (the neural foramina) where the nerve roots leave the spinal canal.Surgeons realized that restoring the normal separation between the vertebrae would open the foramina and take pressure off the nerve roots. Over the last several years, devices called fusion cages have been designed that can be placed between
the vertebrae to hold them apart while the fusion occurs. Enlarging the space between two vertebrae widens the opening of the neural foramina, taking pressure off the spinal nerves that pass through them. The extra space also pulls taut the ligaments inside the spinal canal so they don’t buckle.Fusion cages are made of metal, bone, or graphite material. Some of these cages are shaped like cylinders. They are threaded like a screw on the outside and hollow on the inside. Some are rectangular in shape. The main purpose of the cage, regardless of the shape or material, is to hold the two vertebrae apart while the fusion becomes solid.
Related Document: A Patient’s Guide to Anterior Lumbar Fusion with Cages

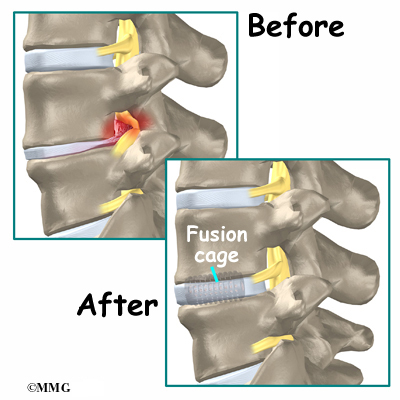
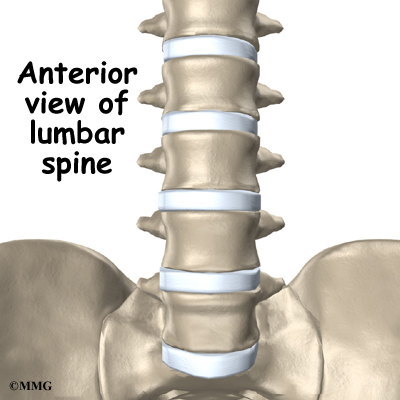{kind=link}
- Posterior Lumbar Interbody Fusion: Finally, surgeons may combine the two methods of anterior fusion and posterior fusion. Fusing both the anterior and posterior portions of the spine gives the most solid fusion. Placing intervertebral cages between the two vertebrae also allows the surgeon to restore the disc height and help take pressure off of the nerve roots that exit at that spinal segment. A common method of doing this is called a posterior lumbar interbody fusion, combined with a posterior lumbar instrumented fusion (described earlier).
Related Document: A Patient’s Guide to Posterior Lumbar Interbody Fusion
Rehabilitation
What should I expect after treatment?
Nonsurgical Rehabilitation
For acute back pain, you may be prescribed two to four weeks of physical therapy. You might need to continue therapy for two to four months for chronic back problems. Treatments are designed to ease pain and to improve your mobility, strength, posture, and function. You’ll also learn how to control your symptoms and how to protect your spine for the years ahead.
At first, your therapist may apply various forms of treatment to address your symptoms. These are especially helpful in the early weeks to improve your comfort so you can get back to your normal activities. You’ll be shown ways to position your spine for maximum comfort while you move, recline, or sleep. To help calm pain and muscle spasm, your therapist may apply heat or ice packs, electrical stimulation, and ultrasound.
If you have severe back pain, your therapist may work with you in a pool. Therapy done in water puts less stress on your low back, and the buoyancy allows you to move easier during exercise.
Hands-on treatments such as massage and specialized forms of soft-tissue mobilization may be used. They can help you begin moving with less pain and greater ease. Medical guidelines also include the early use of spinal manipulation, which has shown short-term benefits in people with acute low back pain. Commonly thought of as an adjustment, spinal manipulation helps reset the sensitivity of the spinal nerves and muscles, easing pain and improving mobility. It involves a high-impulse stretch of the spinal joints and is often characterized by the sound of popping as the stretch is done. It doesn’t provide effective long-term help when used routinely for chronic conditions.
You may be tempted to limit your activity because of your back pain. However, as a result of pain and inactivity, your muscles may become weak and deconditioned, and your back won’t function optimally. Therapists use active rehabilitation to prevent the harmful effects of deconditioning. With this active approach, you’ll be shown how to lift and move safely. And you’ll be shown how to strengthen your back muscles. In addition, aerobic exercises are used to improve your general fitness and endurance.
Aerobic exercises may include walking on a treadmill, riding a stationary bike, or swimming. These activities can relieve the stress of low back pain, and they can cause your body to release endorphins into the blood stream. Endorphins are your body’s own natural painkillers.
An active approach to therapy can help you attain better muscle function, so you can get your activities done easier. Active rehabilitation speeds recovery, reducing the possibility that back pain will become a chronic problem. Activity helps you resume normal activity as swiftly as possible. Though you’ll be cautioned about trying to do too much, too quickly, you’ll be guided toward a return to your usual activities. This approach gives you a greater sense of control. You’ll take an active role in learning how to care for your back pain. Treatment sessions focus on reassuring you that getting back to work and other normal activities swiftly won’t cause you harm and can actually help you get better faster.
When needed, you’ll be encouraged to take certain actions to improve your spine health. For example, if you smoke, you’ll be encouraged to get help to quit. Because of the limited blood supply in the tissues of the low back, smoking speeds the degenerative process and impairs healing. If you’re out of shape, you’ll be encouraged to get fit. This strategy makes it less likely that back pain or injury will strike again in the future.

Your therapist will show you how to keep your spine safe during routine activities. You’ll learn about healthy posture and how posture relates to the future health of your spine. And you’ll learn about body mechanics, how the body moves and functions during activity. Your therapist will also teach safe body mechanics to help you protect your low back as you go about your day. This includes the use of safe positions and movements while lifting and carrying, standing and walking, and performing work duties.
As you recover, you will gradually advance in a series of strengthening exercises for the abdominal and low back muscles. Working these core muscles can help you begin moving easier and lessens the chances of future pain and problems.
As the rehabilitation program evolves, you will progress with more challenging exercises. The goal is to safely advance your strength and function.
Your therapist will work closely with your doctor and employer to help you get back on the job as quickly as reasonably possible. You may be required to do lighter duties at first, but as soon as you are able, you’ll begin doing your normal work activities. Your therapist can also do a work assessment to make sure you’ll be safe to do your job. Your therapist may suggest changes that could help you work safely, with less chance of re-injuring your back.
After Surgery
Rehabilitation after surgery is much more complex. Depending on what operation you’ve had, you may leave the hospital shortly after surgery. Some procedures, such as fusion surgery, require that you stay in the hospital for a few days. When you stay in the hospital, a physical therapist may visit you in your hospital room soon after surgery. Physical therapy sessions help you learn to move and begin doing routine activities without putting extra strain on your low back.

During recovery from surgery, you should follow your surgeon’s instructions about wearing a back brace or soft lumbar support belt. You should be cautious about overdoing activities in the first few weeks after surgery.
You may need therapy outside of the hospital. If you had a lumbar fusion, your surgeon may have you wait six weeks to three months before starting therapy. Once you start in therapy, you’ll usually go for one to three months, depending on your progress and the type of surgery you had.
At first, your therapist may use treatments such as heat or ice, electrical stimulation, massage, and ultrasound to help calm pain and muscle spasm. Pool therapy is often helpful after lumbar surgery.
Exercises are used to improve flexibility in your trunk and lower limbs. Strengthening for your abdominal and low back muscles is started. You’ll be shown safe ways to sleep, sit, lift, and carry. And you’ll be given ideas on how to do your work activities safely.
Ideally, you’ll be able to go back to your previous activities. However, you may need to modify your activities to avoid future problems.
When treatment is well under way, regular visits to the therapist’s office will you’re your therapist will continue to be a resource. But you are in charge of doing your exercises as part of an ongoing home program.
Lumbar Laminectomy
A Patient’s Guide to Lumbar Laminectomy
Introduction
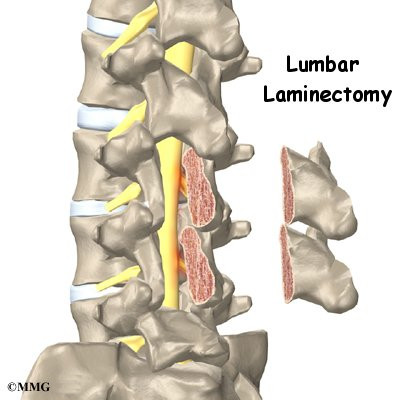
Lumbar laminectomy is a surgical procedure to relieve pressure on the spinal nerves. Degeneration, or wear and tear, in the parts of the spine may narrow the spinal canal. This puts pressure on the nerves in the canal. This condition is called spinal stenosis. A laminectomy involves removing a section of the bony covering over the back of the spinal canal. This takes pressure off the spinal nerves.
This guide will help you understand
- why the procedure becomes necessary
- what surgeons hope to achieve
- what to expect as you recover
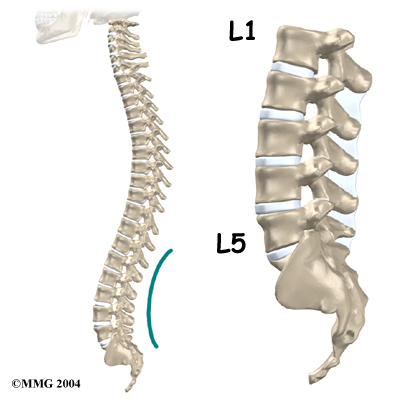
Anatomy
What parts of the spine are involved?
Surgeons perform lumbar laminectomy surgery through an incision in the low back. The surgery involves the pedicle and lamina bones. These bones attach to the back of the spinal column, forming a bony ring that encloses the spinal canal. Surgeons may remove bone spurs from the facet joints
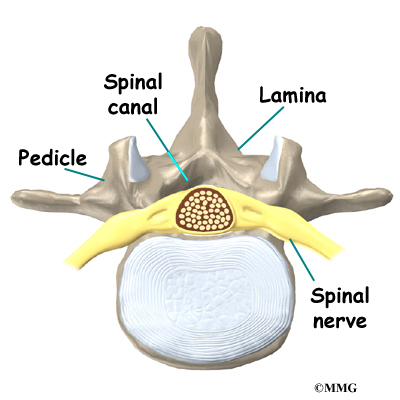
along the back of the spine during the laminectomy procedure, taking pressure off the spinal nerves.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Rationale
What do doctors hope to achieve?
Lumbar laminectomy can alleviate the symptoms of spinal stenosis, a condition in which the spinal nerves become compressed inside the spinal canal. Wear and tear on the spine from aging and from repeated stresses and strains can cause a spinal disc to weaken.
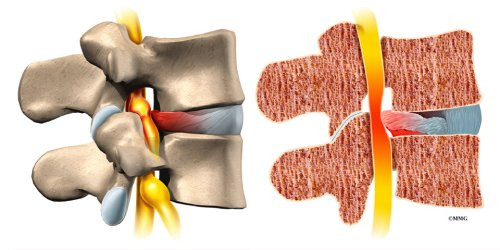
The outer rim of the disc bulges outward, and the disc may eventually protrude or even rupture into the spinal canal, narrowing the size of the canal. As a result, the nerves inside the canal are squeezed, leading to symptoms of spinal stenosis.
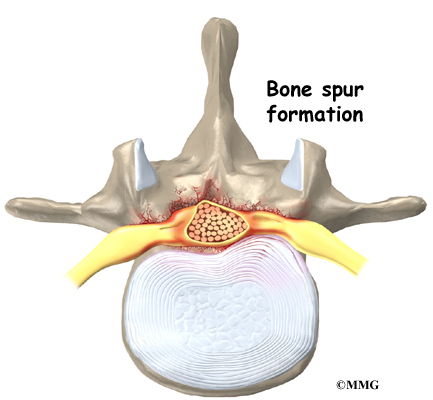
Degeneration also causes bone spurs to develop. These spurs commonly occur around the facet joints and along the edges of the vertebrae. When these spurs point into the spinal canal, they may squeeze against the spinal nerves. In a laminectomy, the surgeon removes a section of the lamina bone and any bone spurs, taking pressure off the spinal nerves. This enlarges the spinal canal so the spinal nerves have more room.
Preparations
How will I prepare for surgery?
The decision to proceed with surgery must be made jointly by you and your surgeon. You should understand as much about the procedure as possible. If you have concerns or questions, talk to your surgeon.
Once you decide on surgery, your surgeon may suggest a complete physical examination by your regular doctor. This exam helps ensure that you are in the best possible condition to undergo the operation.
On the day of your surgery, you will probably be admitted to the hospital early in the morning. You shouldn’t eat or drink anything after midnight the night before.
Surgical Procedure
What happens during the operation?
Patients are given a general anesthesia to put them to sleep during most spine surgeries. As you sleep, your breathing may be assisted with a ventilator. A ventilator is a device that controls and monitors the flow of air to the lungs.
Some surgeons have begun using spinal anesthesia in place of general anesthesia. Spinal anesthesia is injected in the low back into the space around the spinal cord. This numbs the spine and lower limbs. Patients are also given medicine to keep them sedated during the procedure.
This surgery is usually done with the patient kneeling face down in a special frame. The frame supports the patient so the abdomen is relaxed and free of pressure. This position lessens blood loss during surgery and gives the surgeon more room to work.
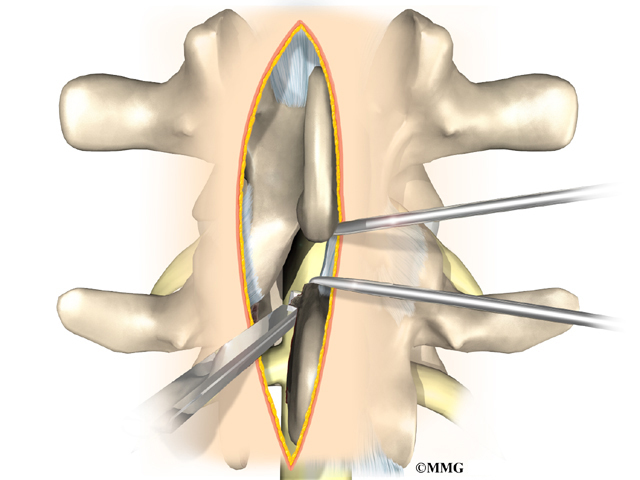
The surgeon makes a short incision down the middle of the low back. The skin and soft tissues are separated to expose the bones along the back of the spine. An X-ray of the low back ensures the surgeon works on the right vertebra. Some surgeons use a special surgical microscope during surgery to magnify the area they’ll be working on.
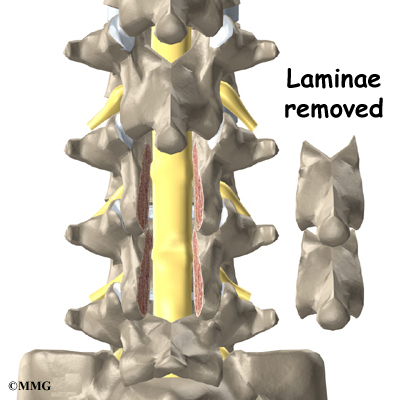
In a complete laminectomy, the spinous process (the bony projection off the back of the vertebra) and the lamina on each side are removed over the area where stenosis is occurring. To accomplish this, the surgeon cuts along the inside edge of the facet joint on each side and detaches the lamina bone completely from the pedicle bones. This opens a section in the bony ring. A small portion of the ligamentum flavum is removed. The ligamentum flavum runs all the way down the spinal canal between the lamina bones and the spinal cord. Removing a small section of this ligament exposes the nerves inside the spinal canal.
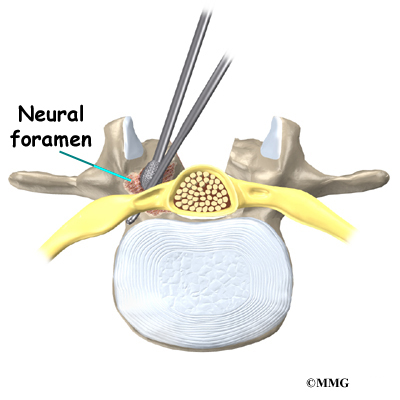
The surgeon may use small cutting instruments to carefully remove soft tissues near the spinal nerves. Then the surgeon takes out any disc fragments and scrapes off nearby bone spurs. In this way, the nerves inside the spinal canal are relieved of additional tension and pressure. The surgeon also enlarges the neural foramina, if needed. The neural foramina are the small openings between the vertebrae where the nerves travel out of the spinal canal.
The muscles and soft tissues are put back in place, and the skin is stitched together.
Complications
What might go wrong?
As with all major surgical procedures, complications can occur. Some of the most common complications following lumbar laminectomy include
- problems with anesthesia
- thrombophlebitis
- infection
- nerve damage
- segmental instability
- ongoing pain
This is not intended to be a complete list of the possible complications.
Problems with Anesthesia
Problems can arise when the anesthesia given during surgery causes a reaction with other drugs the patient is taking. In rare cases, a patient may have problems with the anesthesia itself. In addition, anesthesia can affect lung function because the lungs don’t expand as well while a person is under anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Thrombophlebitis (Blood Clots)
View animation of pulmonary embolism
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can occur after any operation. It occurs when the blood in the large veins of the leg forms blood clots. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lung, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Most surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective is getting you moving as soon as possible. Two other commonly used preventative measures include
- pressure stockings to keep the blood in the legs moving
- medications that thin the blood and prevent blood clots from forming
Infection
Infection following spine surgery is rare but can be a very serious complication. Some infections may show up early, even before you leave the hospital. Infections on the skin’s surface usually go away with antibiotics. Deeper infections that spread into the bones and soft tissues of the spine are harder to treat. They may require additional surgery to treat the infected portion of the spine.
Nerve Damage
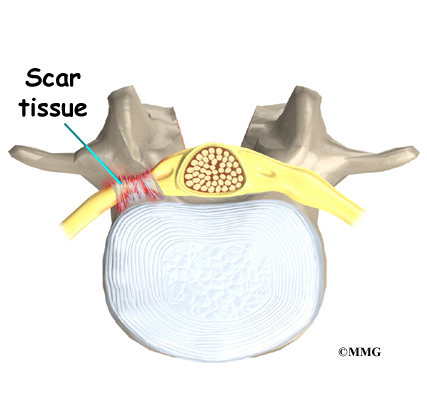
Any surgery that is done near the spinal canal can potentially cause injury to the spinal cord or spinal nerves. Injury can occur from bumping or cutting the nerve tissue with a surgical instrument, from swelling around the nerve, or from the formation of scar tissue. An injury to the spinal cord or spinal nerves can cause muscle weakness and a loss of sensation to the areas supplied by the nerve.
Segmental Instability
Laminectomy surgery can cause the spinal segment to loosen, making it unstable. Each spinal segment includes two vertebrae separated by an intervertebral disc, the nerves that leave the spinal cord at that level, and the small facet joints that link each level of the spinal column.
The facet joints on the back of the spine normally give enough stability, even when the lamina is taken off. This is why surgeons prefer not to remove the facet joints. But these joints may have to be removed if they are enlarged with arthritis or are pushing on the spinal nerves, as explained earlier. When the facet joints must be removed, additional surgery (a fusion) may be needed to fix the loose segment.
Related Document: A Patient’s Guide to Posterior Lumbar Fusion
Ongoing Pain
Many patients get nearly complete relief of symptoms from the lumbar laminectomy procedure. As with any surgery, however, you should expect some pain afterward. If the pain continues or becomes unbearable, talk to your surgeon about treatments that can help control your pain.
After Surgery
What happens after surgery?
Patients are usually able to get out of bed within a few hours after surgery. However, you will be instructed to move your back only carefully and comfortably. Patients are able to return home when their medical condition is stable.
Most patients leave the hospital the day after surgery. They are safe to drive within a week or two. People generally get back to light work by four weeks. Heavier work and sports should wait two to three months. Workers whose jobs involve strenuous manual labor may be counseled to consider different work.
Outpatient physical therapy usually starts four to six weeks after surgery.
Rehabilitation
What should I expect as I recover?
Many surgeons prescribe outpatient physical therapy within six weeks after surgery. Physical therapy after lumbar laminectomy is generally only needed for a total of four to six weeks. You should expect full recovery to take up to four months.
At first, treatments help control pain and inflammation. Ice and electrical stimulation treatments are commonly used to help with these goals. Your therapist may also use massage and other hands-on techniques to ease muscle spasm and pain.
Active treatments are added slowly. These include exercises for improving heart and lung function. Walking and swimming are ideal cardiovascular exercises after lumbar laminectomy surgery. Therapists also teach patients specific exercises to help tone and control the muscles that stabilize the low back.

Your therapist works with you on how to move and do activities. This form of treatment, called body mechanics, is used to help you develop new movement habits. This training helps you keep your back in safe positions as you go about your work and daily activities. At first, this may be as simple as helping you learn how to move safely and easily in and out of bed, how to get dressed and undressed, and how to do some of your routine activities. Then you learn how to keep your back safe while you lift and carry items and as you begin more challenging activities.
As your condition improves, the therapist tailors your program to help prepare you to go back to work. Some patients are not able to go back to a previous job that requires strenuous tasks. Your therapist may suggest changes in job tasks that enable you to go back to your previous job. Your therapist can also suggest alternate forms of work. You’ll learn to do your tasks in ways that keep your back safe and free of extra strain.
Before your therapy sessions end, your therapist will teach you a number of ways to avoid future problems.
Posterior Lumbar Fusion
A Patient’s Guide to Posterior Lumbar Fusion
Introduction
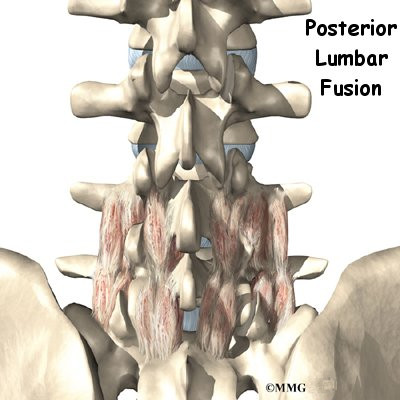
A posterior lumbar fusion is the most common type of fusion surgery for the low back. A fusion is a surgical procedure that joins two or more bones (in this case vertebrae) together into one solid bone. The procedure is called a posterior fusion because the surgeon works on the back, or posterior, of the spine.
Posterior fusion procedures in the lumbar spine are used to treat spine instability, severe degenerative disc disease, and fractures in the lumbar spine.
Other procedures are usually done along with the spinal fusion to take the pressure off nearby nerves. They may include removing bone spurs and injured portions of one or more discs in the low back. Most surgeons also apply metal screws and rods, called instrumentation, to hold the bones securely while they fuse.
This guide will help you understand
- what surgeons hope to achieve
- what happens during the procedure
- what rehabilitation is like after surgery
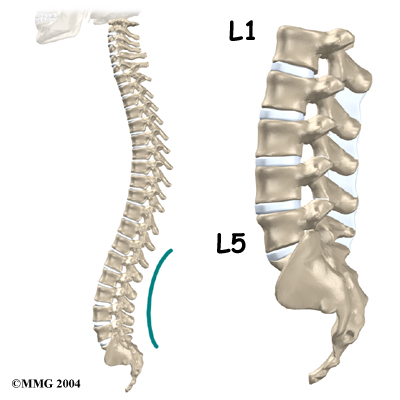
Anatomy
What parts of the back and spine are involved?
Surgeons perform this procedure through an incision in the low back. The incision reaches to the spinous processes, the bony projections off the back of the vertebrae. The surgeon must move aside the muscles along the spine, called the paraspinal muscles. The fusion itself involves the lamina bone, the protective roof over the back surface of the spinal cord.
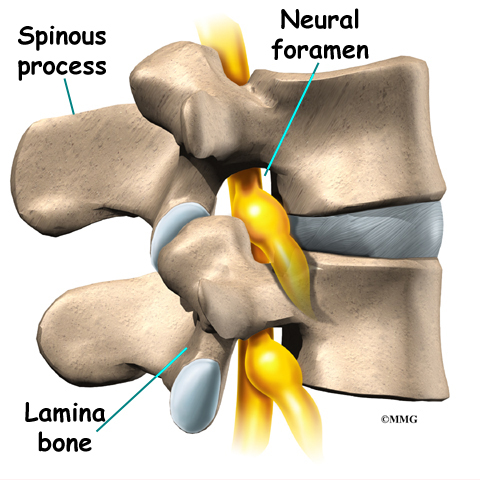
In some cases, the surgeon may enlarge the neural foramina the tunnels where the nerve roots leave the spinal cord.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Rationale
What do surgeons hope to achieve?
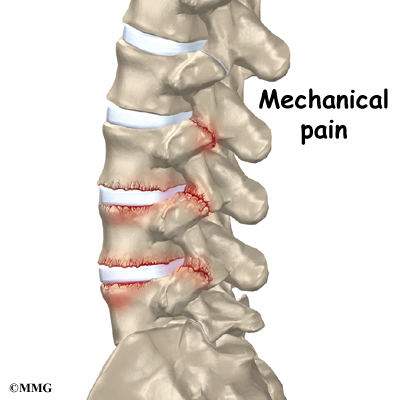
The main goal of the spinal fusion (also known as an arthrodesis) is to stop movement of one or more vertebrae. Keeping the fused section from moving helps stop mechanical pain. Mechanical pain occurs when damaged discs and joints that connect the vertebrae become inflamed from excessive motion between the vertebrae. This type of pain is commonly felt in the low back and may radiate into the buttocks and upper thighs.
The spinal nerves are also affected by too much vertebral motion. They begin to rub
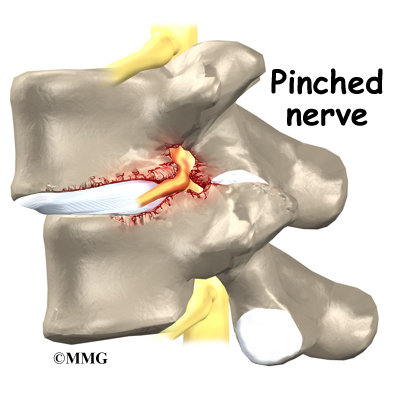
where they pass through the neural foramina and become swollen and irritated. Also, the neural foramina narrow when a vertebra slides too far forward or backward over the vertebra below. This immediately pinches the nerves where they pass through the neural foramina. Nerve swelling, irritation, and pinching produce neurogenic pain. This type of pain often radiates down one or both legs below the knee. Fusion stops this harm to the nerves.
By fusing the vertebrae together, surgeons hope to slow down the process of degeneration at the fused segments and prevent future problems.
Preparations
How will I prepare for surgery?
The decision to proceed with surgery must be made jointly by you and your surgeon. You should understand as much about the procedure as possible. If you have concerns or questions, talk to your surgeon.
Once you decide on surgery, your surgeon may suggest a complete physical examination by your regular doctor. This exam helps ensure that you are in the best possible condition to undergo the operation.
On the day of your surgery, you will probably be admitted to the hospital early in the morning. You shouldn’t eat or drink anything after midnight the night before.
Surgical Procedure
What happens during the operation?
Patients are given a general anesthesia to put them to sleep during most spine surgeries. As you sleep, your breathing may be assisted with a ventilator. A ventilator is a device that controls and monitors the flow of air to the lungs.
During surgery the patient usually kneels face down on a special operating table. The special table supports the patient so the abdomen is relaxed and free of pressure. This position lessens blood loss during surgery. It also gives the surgeon more room to work.
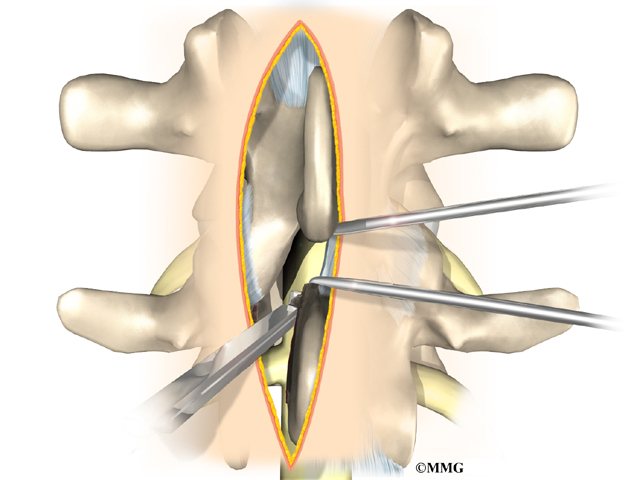
An incision is made down the middle of the low back. The tissues just under the skin are separated. Then the small muscles along the sides of the low back are lifted off the vertebrae, exposing the back of the spinal column. Next, the surgeon takes an X-ray to make sure that the procedure is being performed on the correct vertebrae.
The surgeon first removes any pressure from nearby nerves. This may involve removing part or all of the lamina bone. (The lamina forms the back portion of the bony ring covering the spinal canal.) Then the surgeon takes out any disc fragments and scrapes off nearby bone spurs. In this way, the nerves inside the spinal canal are relieved of additional tension and pressure. The nerve roots are checked to see if they move freely in the spinal canal and as they leave the spine through the small holes between the vertebrae, the neural foramina. If not, the surgeon may cut a larger opening in the neural foramina. This procedure is called foraminotomy.
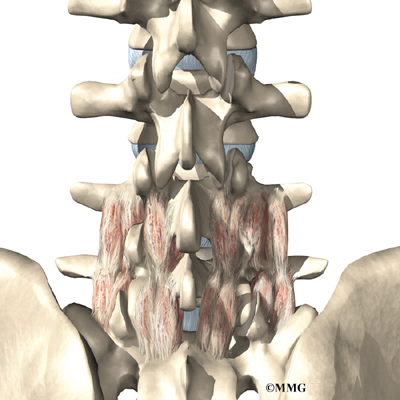
To prepare the area to be fused, the surgeon shaves a layer of bone off the back surfaces of the spinal column. The cut bone bleeds. The surgeon makes a second incision at the hip. Small strips of bone are removed from the top rim of the pelvis. This is called a bone graft. The surgeon lays the bone strips over the back of the spinal column. When the bone graft contacts the bleeding area, the body heals (or fuses) the bones together just as it would a fractured bone.
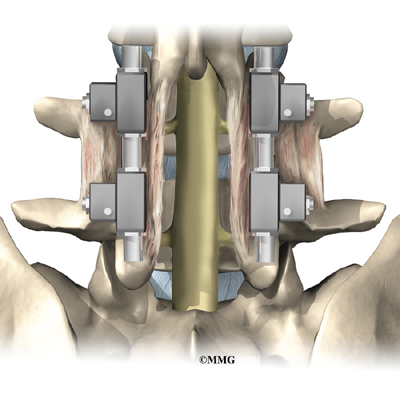
During posterior spinal fusion, the surgeon also fixes the bones in place using a combination of metal screws, rods, and plates. This instrumentation (or hardware, as it is sometimes called) holds the vertebrae to be fused together and prevents them from moving. The less motion there is between two bones trying to heal, the higher the chance they will successfully fuse. The use of instrumentation has increased the success rate of spinal fusions considerably.
A drainage tube may be placed in the wound. The muscles and soft tissues are put back in place, and the skin is stitched together. The surgeon may place you in a rigid brace to support your spine while it heals.
Complications
What might go wrong?
As with all major surgical procedures, complications can occur. Some of the most common complications following posterior lumbar fusion include
- problems with anesthesia
- thrombophlebitis
- infection
- nerve damage
- problems with the graft or hardware
- muscle disruption
- nonunion
- ongoing pain
This is not intended to be a complete list of the possible complications.
Problems with Anesthesia
Problems can arise when the anesthesia given during surgery causes a reaction with other drugs the patient is taking. In rare cases, a patient may have problems with the anesthesia itself. In addition, anesthesia can affect lung function because the lungs don’t expand as well while a person is under anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Thrombophlebitis (Blood Clots)
View animation of pulmonary embolism
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can occur after any operation. It occurs when the blood in the large veins of the leg forms blood clots. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lung, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Most surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective is getting you moving as soon as possible. Two other commonly used preventative measures include
- pressure stockings to keep the blood in the legs moving
- medications that thin the blood and prevent blood clots from forming
Infection
Infection following spine surgery is rare but can be a very serious complication. Some infections may show up early, even before you leave the hospital. Infections on the skin’s surface usually go away with antibiotics. Deeper infections that spread into the bones and soft tissues of the spine are harder to treat. They may require additional surgery to treat the infected portion of the spine.
Nerve Damage
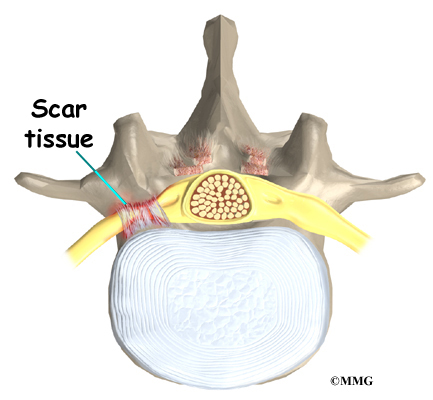
Any surgery that is done near the spinal canal can potentially cause injury to the spinal cord or spinal nerves. Injury can occur from bumping or cutting the nerve tissue with a surgical instrument, from swelling around the nerve, or from the formation of scar tissue. An injury to these structures can cause muscle weakness and a loss of sensation to the areas supplied by the nerve.
Problems with the Graft or Hardware
Posterior fusion surgery requires bone to be grafted onto the spinal column. The graft is commonly taken from the top rim of the pelvis. There is a risk of pain, infection, or weakness in the area where the graft is taken.
Sometimes the strips of bone graft don’t take and end up dissolving. A second surgery may be needed to remove the strips and apply more graft material. The doctor may need to apply additional metal hardware to hold the new grafts firmly in place.
When instrumentation is used, the screws, rods, or plates can also cause problems. They can loosen and irritate the nearby soft tissues. In rare cases, they may actually break. If your hardware loosens or breaks, the surgeon may suggest another surgery either to take out the hardware or to add more hardware to solve the problem.
Muscle Disruption
During the operation, the surgeon lifts off the small muscles that run along the back of the spinal column. Some of the nerves going to the muscles are cut. Lifting the muscles away from the bone impairs the blood supply to the muscles. Disruption of the nerve and blood supply can cause the muscles to fatigue easily, especially during a long work day and with heavy or repeated lifting. Exercises designed by a physical therapist boost strength and endurance in the nearby muscles, reducing symptoms from this problem.
Nonunion
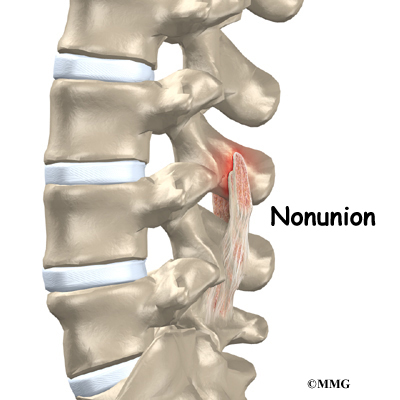
Sometimes the bones do not fuse as planned. This is called a nonunion or pseudarthrosis. (The term pseudarthrosis means false joint.) When more than one level of the spine is fused at one time, there is a greater chance that nonunion will occur. Fusion of more than one level means that two or more consecutive discs are removed and replaced with bone graft. If the joint motion from a nonunion causes pain, you may need a second operation.
In the second procedure, the surgeon usually adds more bone graft. Metal plates and screws may also be added to rigidly secure the bones so they will fuse together.
Ongoing Pain
Posterior lumbar fusion is a complex surgery. Not all patients get complete pain relief with this procedure. Successful fusion occurs in more than 80 percent of surgeries. But a solid fusion does not guarantee freedom from pain or the ability to return to normal activity. If you have pain that continues or becomes unbearable, talk to your surgeon about treatments that can help control your pain.
After Surgery
What happens after surgery?
Patients may be placed in a rigid body brace after surgery. This brace may not be needed if the surgeon attached metal hardware to the spine during the surgery. The drain tube is removed from the wound within 24 to 48 hours.
Patients usually stay in the hospital after surgery for up to one week. During this time, a physical therapist helps patients learn safe ways to move, dress, and do activities without putting extra strain on the back. Patients may be instructed to use a walker for the first day or two. Before going home, patients are shown how to help control pain and avoid problems.
Patients are able to return home when their medical condition is stable. However, they are usually required to keep their activities to a minimum in order to give the graft time to heal. Patients should avoid bending, lifting, twisting, driving, and prolonged sitting for up to six weeks. Outpatient physical therapy usually starts a minimum of six weeks after surgery.
Patients gradually do more activities and exercise with the goal of getting back to a normal and productive life.
Rehabilitation
What should I expect as I recover?
Rehabilitation after posterior lumbar fusion can be a slow process. Many surgeons prescribe outpatient physical therapy beginning a minimum of six weeks after surgery. This delay is needed to make sure the fusion is taking. You will probably need to attend therapy sessions for two to three months. You should expect full recovery to take up to eight months. Therapy can usually progress faster in patients who had an instrumented fusion.
At first, treatments help control pain and inflammation. Ice and electrical stimulation treatments are commonly used to help with these goals. Your therapist may also use massage and other hands-on techniques to ease muscle spasm and pain.

Active treatments are slowly added. These include exercises for improving heart and lung function. Short, slow walks are generally safe to start with after posterior lumbar fusion. Swimming and use of a stair-climbing machine are helpful in the later phases of treatment. Therapists also teach patients specific exercises to help tone and control the muscles that stabilize the low back.
Your therapist also works with you on how to move and do activities. This form of treatment, called body mechanics, is used to help you develop new movement habits. This training helps you keep your back in safe positions as you go about your work and daily activities. Training includes positions you use when sitting, lying, standing, and walking. You’ll also work on safe body mechanics for lifting, carrying, pushing, and pulling.
As your condition improves, the therapist tailors your program to help prepare you to go back to work. Some patients are not able to go back to a previous job that requires strenuous tasks. Your therapist may suggest changes in job tasks that enable you to go back to your previous job or to do alternate forms of work. You’ll learn to do these tasks in new ways that keep your back safe and free of strain.
Before your therapy sessions end, your therapist will teach you how to avoid future problems.
Lumbar Spinal Stenosis
A Patient’s Guide to Lumbar Spinal Stenosis
Introduction

According to the North American Spine Society (NASS), spinal stenosis describes a clinical syndrome of buttock or leg pain. These symptoms may occur with or without back pain. It is a condition in which the nerves in the spinal canal are closed in, or compressed. The spinal canal is the hollow tube formed by the bones of the spinal column. Anything that causes this bony tube to shrink can squeeze the nerves inside. As a result of many years of wear and tear on the parts of the spine, the tissues nearest the spinal canal sometimes press against the nerves. This helps explain why lumbar spinal stenosis (stenosis of the low back) is a common cause of back problems in adults over 55 years old.
This guide will help you understand
- how the problem develops
- how doctors diagnose the condition
- what treatment options are available
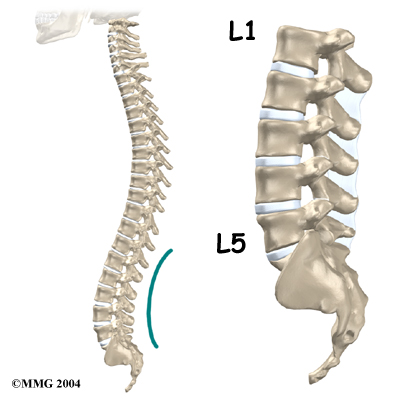
Anatomy
What part of the back is involved?
The human spine is made up of 24 spinal bones, called vertebrae. Vertebrae are stacked on top of one another to create the spinal column. The spinal column gives the body its form. It is the body’s main upright support.
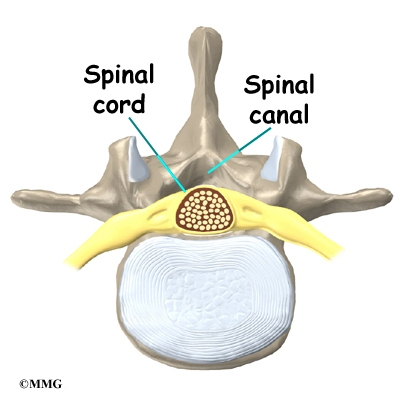
The back portion of the spinal column forms a bony ring. When the vertebrae are stacked on top of each other, these bony rings create a hollow tube. This bony tube, called the spinal canal, surrounds the spinal cord as it passes through the spine. Just as the skull protects the brain, the bones of the spinal column protect the spinal cord.
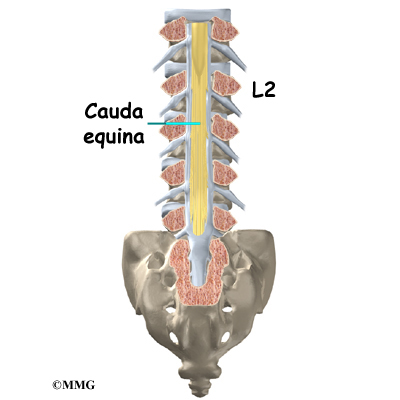
The spinal cord only extends to the second lumbar (low back) vertebra. Below this level, the spinal canal encloses a bundle of nerves that go to the lower limbs and pelvic organs. The Latin term for this bundle of nerves is cauda equina, meaning horse’s tail.
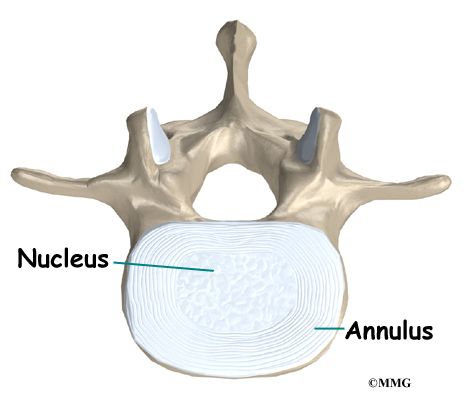
An intervertebral disc fits between each vertebral body and provides a space between the spine bones. The disc normally works like a shock absorber. It protects the spine against the daily pull of gravity. It also protects the spine during heavy activities that put strong force on the spine, such as jumping, running, and lifting.
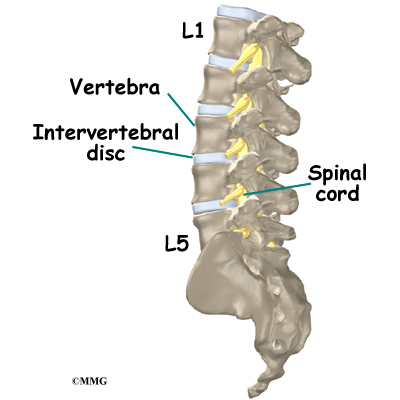
An intervertebral disc is made up of two parts. The center, called the nucleus, is spongy. It provides most of the ability to absorb shock. The nucleus is held in place by the annulus, a series of strong ligament rings surrounding it. Ligaments are strong connective tissues that attach bones to other bones.
Related Document: A Patient’s Guide to Lumbar Spine Anatomy
Causes
Why do I have this problem?
In the lumbar spine, the spinal canal usually has more than enough room for the spinal nerves. The canal is normally 17 to 18 millimeters around, slightly smaller than a penny. Spinal stenosis develops when the canal shrinks to 12 millimeters or less. When the size drops below 10 millimeters, severe symptoms of lumbar spinal stenosis occur.
There are many reasons why symptoms of spinal stenosis develop. Some of the more common reasons include
- congenital stenosis (being born with a small spinal canal)
- spinal degeneration
- spinal instability
- disc herniation
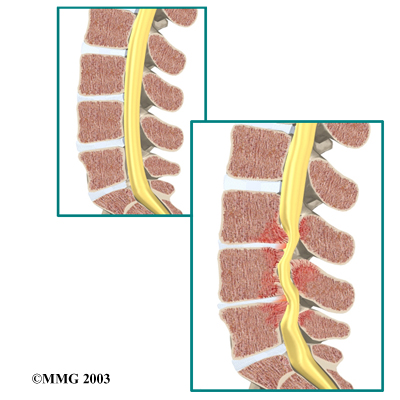
Congenital stenosis: Some people are born with (congenital) a spinal canal that is narrower than normal. They may not feel problems early in life. However, having a narrow spinal canal puts them at risk for stenosis. Even a minor back injury can cause pressure against the spinal cord. People born with a narrow spinal canal often have problems later in life, because the canal tends to become narrower due to the effects of aging.
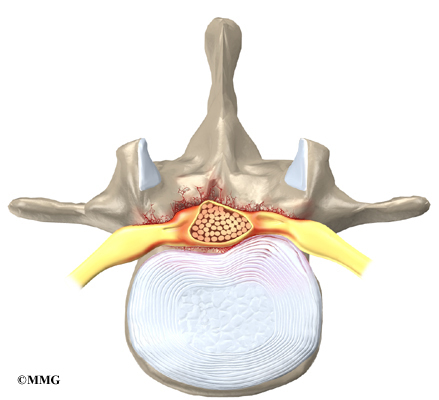
Degeneration: Degeneration is the most common cause of spinal stenosis. Wear and tear on the spine from aging and from repeated stresses and strains can cause many problems in the lumbar spine. The intervertebral disc can begin to collapse, and the space between each vertebrae shrinks. Bone spurs may form that stick into the spinal canal and reduce the space available to the spinal nerves. The ligaments that hold the vertebrae together may thicken and also push into the spinal canal. All of these conditions cause the spinal canal to narrow.
View animation of degeneration
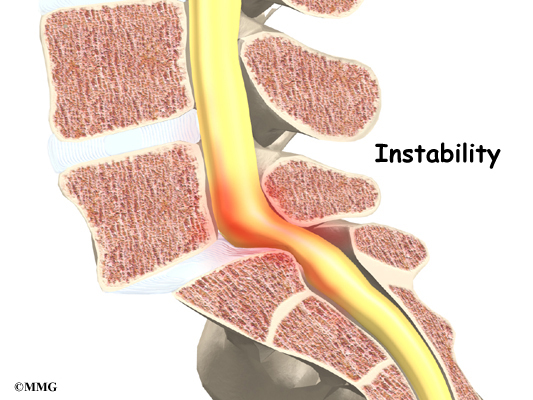
Spinal instability: Spinal instability can cause spinal stenosis. Spinal instability means that the bones of the spine move more than they should. Instability in the lumbar spine can develop if the supporting ligaments have been stretched or torn from a severe back injury. People with diseases that loosen their connective tissues may also have spinal instability. Whatever the cause, extra movement in the bones of the spine can lead to spinal stenosis.
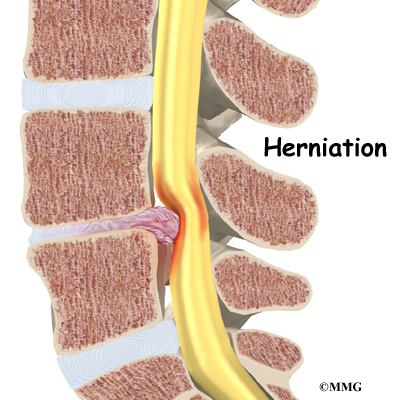
Disc herniation: Spinal stenosis can occur when an intervertebral disc in the low back herniates (ruptures). Normally, the shock-absorbing disc is able to handle the downward pressure of gravity and the strain from daily activities. However, if the pressure on the disc is too strong, such as landing from a fall in a sitting position, the nucleus inside the disc may rupture through the outer annulus and squeeze out of the disc. This is called a disc herniation. If an intervertebral disc herniates straight backward, it can press against the nerves in the spinal canal, causing symptoms of spinal stenosis.
Symptoms
What does the spinal stenosis feel like?
Spinal stenosis usually develops slowly over a long period of time. This is because the main cause of spinal stenosis is spinal degeneration in later life. Symptoms rarely develop quickly when degeneration is the source of the problem. A severe injury or a herniated disc may cause symptoms to develop immediately.
Patients with stenosis don’t always feel back pain. Primarily, they have severe pain and weakness in their legs, usually in both legs at the same time. Some people say they feel that their legs are going to give out on them.
Symptoms mainly affect sensation in the lower limbs. Nerve pressure from stenosis can cause a feeling of pins and needles in the skin where the spinal nerves travel. Reflexes become slowed. Some patients report charley horses in their leg muscles. Others report strange sensations like water trickling down their legs.
Symptoms change with the position of the low back. Flexion (bending forward) widens the spinal canal and usually eases symptoms. That’s why people with stenosis tend to get relief when they sit down or curl up to sleep. Activities such as reaching up, standing, and walking require the spine to straighten or even extend (bend back slightly). This position of the low back makes the spinal canal smaller and often worsens symptoms.
Diagnosis
How do doctors diagnose the problem?
Diagnosis begins with a complete history and physical examination. Your doctor will ask questions about your symptoms and how your problem is affecting your daily activities. This will include questions about your pain or if you have feelings of numbness or weakness in your legs.
Your doctor will also want to know whether your symptoms are worse when you’re up standing or walking and if they go away when you sit down. If your pain does not get worse when walking, then you probably don’t have stenosis. There may be some other cause of the painful symptoms.
The doctor does a physical examination to see which back movements cause pain or other symptoms. Your skin sensation, muscle strength, and reflexes are also tested. A wide-based gait (legs far apart) is often observed. Special clinical tests can be done such as the Romberg test, hip extension test, and tests of neuromuscular function.
The Romberg test is a neurologic test for joint proprioception (sense of position). The nerve pathways for this sensation travel up the dorsal columns of the spinal cord. Dorsal means they are located towards the back where stenosis is more likely to occur. The test is done standing with feet together, eyes open, and hands by your sides. You will be asked to close your eyes for one full minute while your doctor observes you. Romberg’s test is positive if you can stand with your eyes open but fall (or start to fall, someone will be there to make sure you don’t fall down) when your eyes are closed. The test is not positive if you start to sway with your eyes closed but don’t lose your balance.
X-rays can show if the problems are from changes in the bones of the spine. The images can show if degeneration has caused the space between the vertebrae to collapse. X-rays may also show any bone spurs sticking into the spinal canal.
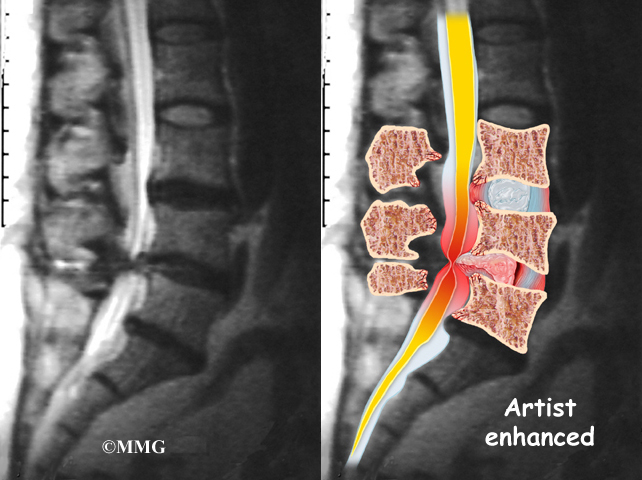
The best way to see the effects and extent of lumbar spinal stenosis is with a magnetic resonance imaging (MRI) scan. The MRI machine uses magnetic waves rather than X-rays to show the soft tissues of the body. This test gives a clear picture of the spinal canal and whether the nerves inside are being squeezed. This machine creates pictures that look like slices of the area your doctor is interested in. The test does not require dye or a needle.
Computed tomography (a CT scan) may be ordered for those patients who can’t have an MRI for some reason, when the results of the MRI are unclear, or symptoms don’t match the MRI findings. The CT scan is a detailed X-ray that lets your doctor see slices of bone tissue. The image can show any bone spurs that may be sticking into the spinal column and taking up space around the spinal nerves.

When there is a concern about neurologic problems, doctors may recommend electrodiagnostic tests of the nerves that go to the legs and feet. An electromyogram (EMG) checks whether the motor pathway of a nerve is working correctly. Motor impulses travel down the nerve and work to energize muscles.
Doctors may also order a somatosensory evoked potential (SSEP) test to locate more precisely where the spinal nerves are being squeezed. The SSEP is used to measure nerve sensations. These sensory impulses travel up the nerve, informing the body about sensations such as pain, temperature, and touch. The function of a nerve is recorded by an electrode placed over the skin in the area where the nerve travels.
Not all causes of spinal stenosis are from degenerative conditions. Doctors use blood tests to determine whether symptoms are coming from other conditions, such as arthritis or infection.
Treatment
What treatment options are available?
Nonsurgical Treatment
Unless your condition is causing significant problems or is rapidly getting worse, most doctors will begin with nonsurgical treatments. Up to one-half of all patients with mild-to-moderate lumbar spinal stenosis can manage their symptoms with conservative (nonsurgical) care. Neurologic decline and paralysis in this group is rare.
At first, doctors may prescribe ways to immobilize the spine. Keeping the back still for a short time can calm inflammation and pain. This might include one to two days of bed rest. Patients may find that curling up to sleep or lying back with their knees bent and supported gives the greatest relief. These positions flex the spine forward, which widens the spinal canal and can ease symptoms.
A lumbar support belt or corset may be prescribed, though their benefits are controversial. Lumbosacral corsets do not appear to offer any long-term benefits. The support provides symptom relief only while you are wearing it. The support can limit pressure in the discs and prevent extra movement in the spine. But it can also cause the back and abdominal muscles to weaken. Some doctors have their patients wear a rigid brace that holds the spine in a slightly flexed position, widening the spinal canal. Health care providers normally only have patients wear a corset for one to two weeks.
Doctors sometimes prescribe medication for patients with spinal stenosis. Patients may be prescribed anti-inflammatory medication such as nonsteroidal anti-inflammatory drugs (NSAIDs) or aspirin. These medications can cause side effects in the kidneys and gastrointestinal tract. Also, because most stenosis patients are elderly, doctors closely monitor patients who are using these medications to avoid complications.
Narcotic drugs, such as codeine or morphine, are generally not prescribed for stenosis patients. They are addictive when used too much or improperly. Muscle relaxants are occasionally used to calm muscles in spasm.
Symptoms of stenosis can lead to mood changes. As a result, doctors sometimes prescribe anti-depressant medication, called tricyclics. Tricyclics help steady peoples’ moods, and some tricyclics even improve sleep by helping the body make an important hormone called serotonin. These medications also seem to calm back pain by affecting the membranes around pain nerves.
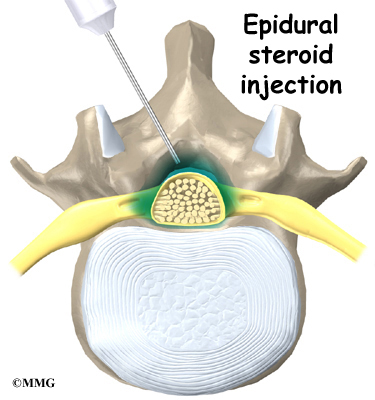
Some patients are given an epidural steroid injection (ESI). The spinal cord is covered by a material called dura. The space between the dura and the spinal column is called the epidural space. It is thought that injecting steroid medication into this space fights inflammation around the nerves, the discs, and the facet joints. This can reduce swelling and give the nerves more room inside the spinal canal.
Research shows that a single steroid injection offers only short-term relief. Multiple injections can produce long-term, lasting pain relief. Epidural injections should be given using contrast-enhanced fluoroscopy. Fluoroscopy is an imaging technique used by the surgeon to guide the needle to the right spot during the procedure. This type of imaging improves the accuracy of medication delivery.
Patients often work with a physical therapist. By evaluating your condition, your therapist can assign positions and exercises to ease your symptoms. Your therapist may suggest using traction. Traction is a common treatment for stenosis. It gently stretches the low back, taking pressure off the spinal nerves. Your therapist may also suggest strengthening and aerobic exercises. Strengthening exercises focus on improving the strength and control of the back and abdominal muscles. Aerobic exercises are used to improve heart and lung health and increase endurance in the spinal muscles. Stationary biking offers a good aerobic treatment and keeps the spine bent slightly forward, a position affording relief to many patients with lumbar stenosis.
Surgery
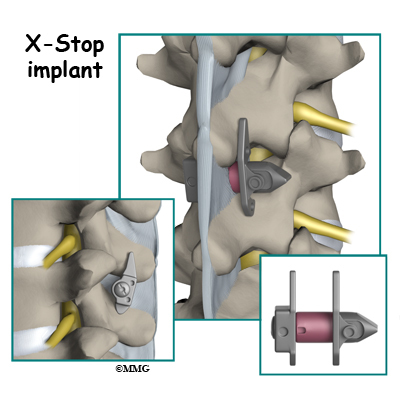
If the symptoms you feel are mild and there is no danger they’ll get worse, surgery is not usually recommended. Some patients may benefit from the use of a device called the X-STOP®. The X-STOP® is a metal implant made of titanium. The implant is inserted through a small incision in the skin of your back. It is designed to fit between the spinous processes of the vertebrae in your lower back. It stays in place permanently without attaching to the bone or ligaments in your back.
There are several advantages of the X-STOP®. It can be inserted using local anesthesia on an outpatient basis. A small incision is made so the procedure is minimally invasive and no bone or soft tissue is removed. The implant is not close to nerves or the spinal cord. With the implant in place, you won’t have to bend forward to relieve your symptoms. The X-STOP® keeps the space between your spinous processes open. With the implant in place, you stand upright without pinching the nerves in your back.
But for anyone with severe symptoms of lumbar spinal stenosis, surgery may be needed. When there are signs that pressure is building on the spinal nerves, decompressive surgery may be required, sometimes right away. Decompression means that bone and/or soft tissue are removed from around the spinal nerves to take the pressure off. The signs doctors watch for when reaching this decision include weakening in the leg muscles, pain that won’t ease up, and problems with the bowels or bladder.
Pressure on the spinal nerves can cause a loss of control in the bowels or bladder. This is an emergency. If the pressure isn’t relieved, it can lead to permanent paralysis of the bowels and bladder. Surgery is recommended to remove pressure from the nerves.
The main surgical procedure used to treat spinal stenosis is lumbar laminectomy. Some patients also require fusion surgery immediately after the laminectomy procedure if spinal instability is present.
Lumbar Laminectomy

The lamina is the covering layer of the bony ring of the spinal column. It forms a roof-like structure over the back of the spinal canal. When the nerves in the spinal canal are being squeezed by a herniated disc or bone spurs, a lumbar laminectomy removes the entire lamina to release pressure on the spinal nerves. This is the primary type of surgery used for lumbar spinal stenosis.
Related Document: A Patient’s Guide to Lumbar Laminectomy
Posterior Lumbar Fusion
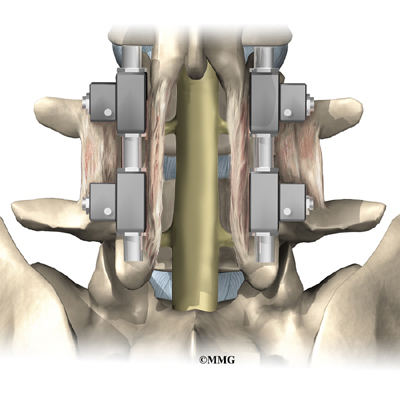
A posterior lumbar fusion may be needed after a surgeon performs a lumbar laminectomy. The fusion procedure is recommended when a spinal segment has become loose or unstable.
A fusion surgery joins two or more bones into one solid bone. This keeps the bones and joints from moving. In this procedure, the surgeon lays small grafts of bone over the back of the spine. Most surgeons also apply metal plates and screws to prevent the two vertebrae from moving.
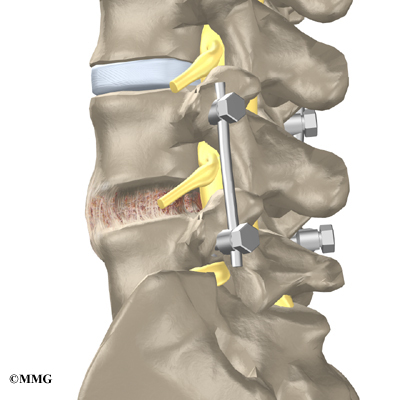
This protects the graft so it can heal better and faster.
Related Document: A Patient’s Guide to Posterior Lumbar Fusion
Rehabilitation
What should I expect as I recover?
Nonsurgical Rehabilitation
Even if you don’t need surgery, your doctor may recommend that you work with a physical or occupational therapist. Patients are normally seen a few times each week for one to two months. In severe cases, patients may need a few additional weeks of care.
Your therapist creates a program to help you regain back movement, strength, endurance, and function. Treatments for lumbar spinal stenosis often include lumbar traction, described earlier. Hands-on treatments such as massage and specialized forms of soft-tissue mobilization may be used initially. They are used to help you begin moving with less pain and greater ease. Therapists also guide patients in a program of exercise designed to widen the spinal canal and take pressure off the spinal nerves.
It is important to improve the strength and coordination in the abdominal and low back muscles. Your therapist can also evaluate your workstation or the way you use your body when you do your activities and suggest changes to avoid further problems.
After Surgery
After surgery, surgeons may have their patients work with a physical or occupational therapist. Patients who’ve had fusion surgery normally need to wait two to three months before beginning a rehabilitation program. They will probably need to attend therapy sessions for six to eight weeks and should expect full recovery to take up to six months.
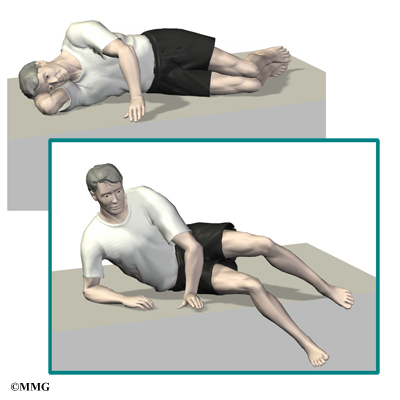
During therapy after surgery, the therapist may use treatments such as heat or ice, electrical stimulation, and massage to help calm pain and muscle spasm. Then patients begin learning how to move safely with the least strain on their healing back.
As the rehabilitation program evolves, patients do more challenging exercises. The goal is to safely advance strength and function. As the therapy sessions come to an end, therapists help patients get back to the activities they enjoy.

Ideally, patients are able to resume normal activities. Patients may need guidance on which activities are safe or how to change the way they go about certain activities.
When treatment is well under way, regular visits to the therapist’s office will end. The therapist will continue to be a resource. But patients are in charge of doing their exercises as part of an ongoing home program.