A Patient’s Guide to Snapping Scapula Syndrome
Introduction
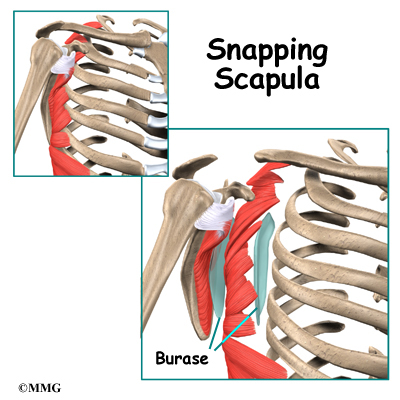
The scapulothoracic joint is located where the shoulder blade (also called the scapula) glides along the chest wall (the thorax). When movement of this joint causes feelings or sounds of grating, grinding, popping, or thumping, doctors call it snapping scapula syndrome.
Snapping scapula syndrome is fairly rare. When it happens, the soft tissues between the scapula and the chest wall are thick, irritated, or inflamed. Snapping scapula syndrome can also happen if the bones of the shoulder blade or rib cage grate over one another.
This guide will help you understand
- what causes snapping scapula syndrome
- how doctors treat this condition
Anatomy
What parts of the body are involved in this condition?
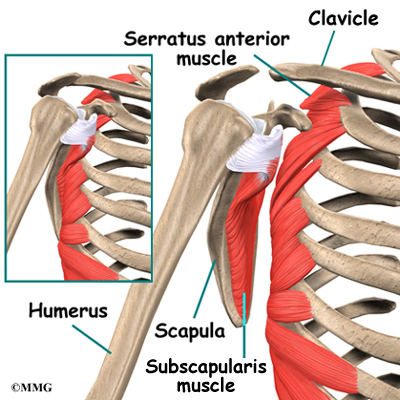
The shoulder is made up of three bones: the humerus (upper arm bone), the clavicle (collarbone), and the scapula (shoulder blade). Two large muscles attach to the front part of the scapula where it rests against the chest wall. One of them, called the subscapularis muscle, attaches over the front of the scapula where it faces the chest wall. The serratus anterior muscle attaches along the edge of the scapula nearest the spine. It passes in front of the scapula, wraps around the chest wall, and connects to the ribs on the front part of the chest.
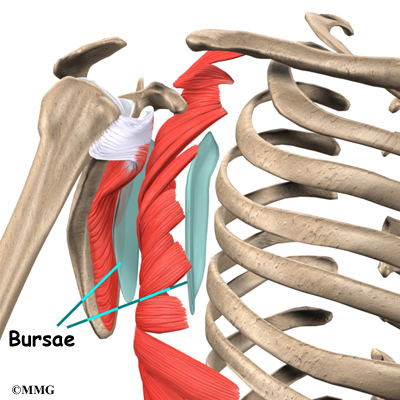
A bursa is a fluid-filled sac that cushions body tissues from friction. A bursa sits between the two muscles of the scapula. There is also a bursa in the space between the serratus anterior muscle and the chest wall. When bursa sacs become inflamed, the condition is called bursitis.
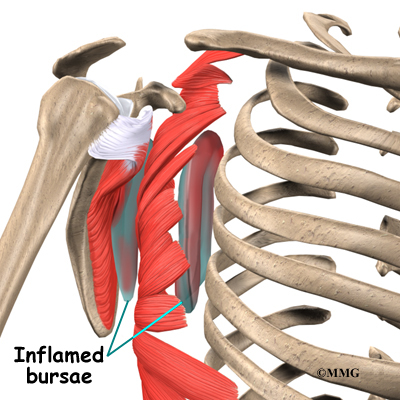
Scapulothoracic bursitis refers to inflammation in the bursa under the shoulder blade. This type of bursitis is most common in the upper corner of the scapula nearest the spine. It also occurs under the lower tip of the scapula. In either case, it can cause the sounds and sensations of snapping scapula syndrome. A person can have bursitis in the joint without any grinding or popping.
Related Document: A Patient’s Guide to Shoulder Anatomy
Causes
What causes this condition?
Snapping scapula is caused by problems in the soft tissues or bones of the scapula and chest wall. It can start when the tissues between the scapula and shoulder blade thicken from inflammation. The inflammation is usually caused by repetitive movements. Certain motions of the shoulder done over and over again, such as the movements of pitching baseballs or hanging wallpaper, can cause the tissues of the joint to become inflamed.
In other cases, the muscles under the scapula have shrunk (atrophied) from weakness or inactivity. The scapula bone then rides more closely to the rib cage. This means the scapula bumps or rubs on the rib bones during movement.
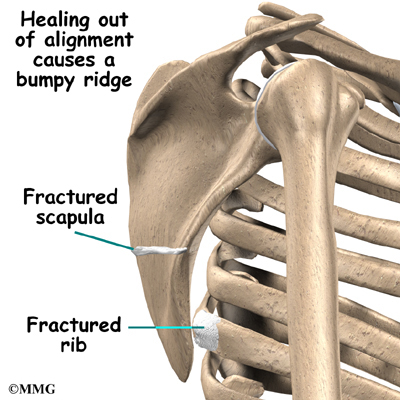
Changes in the alignment or contour of the bones of the scapulothoracic joint can also cause snapping scapula. When a fractured rib or scapula isn’t lined up just right, it can cause a bumpy ridge that produces the characteristic grind or snap as the scapula moves over the chest wall.
Grinding and snapping can also happen if there are any abnormal curves, bumps, or ledges on the upper edge of the scapula closer to the center of the back. (These abnormalities are called Luschka’s tubercles.) Any time there is an abnormality in the bone, one of the body’s possible responses is to form a bursa. The new bursa may then become inflamed, causing the symptoms of bursitis.
Symptoms
What symptoms does snapping scapula cause?
Grating, grinding, or snapping may be heard or felt along the edge or undersurface of the scapula as it moves along the chest wall. These grinding sensations are also called crepitus. Sometimes the joint pops or thumps during movement. Often, these sensations cause no pain.
Scapulothoracic bursitis, on the other hand, is painful whether or not there is any crepitus in the joint. The sore bursa is usually tender to the touch, and the tissue in the sore area often feels thick.
Diagnosis
What tests will the doctor run?
Your doctor will ask many questions about your medical history. The goal is to find out if you’ve had similar problems in the past, if you’ve injured your scapula, and if any of your activities require repetitive shoulder movements.
Your doctor will also do a physical exam. He or she will check the alignment of the scapula. Your doctor may listen with a stethoscope while you move your shoulder and scapula. You may feel pain as you move, but it is important that your doctor knows exactly where your problem is coming from. By feeling the tissues around the scapula, your doctor can find out if the bursa is tender or thickened from inflammation.
Your doctor may order an X-ray to see between the scapula and rib cage. An X-ray image can show abnormalities in the bone, such as a rib or scapular fracture. In cases where there may be a problem with the bones, your doctor may order a computed tomography (CT) scan to get a more detailed look. If bursitis is suspected, a magnetic resonance imaging (MRI) may be used to locate the bursa and see how big it is. MRI scans use magnetic waves to show the soft tissues of the body in slices.
Treatment
What treatment options are available?
Nonsurgical Treatment
Most doctors prescribe nonsurgical treatments for patients with snapping scapula. These types of treatments are generally successful, especially when the problem is coming from soft tissues. Doctors may start by prescribing nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin and ibuprofen. Rest and ice also help reduce inflammation and ease pain. Some patients benefit by working with a physical or occupational therapist.
If pain and inflammation don’t go away with these treatments, your doctor may recommend one or two injections of cortisone into the bursa. Cortisone is a steroid that effectively reduces inflammation.
Related Document: A Patient’s Guide to Joint Injections for Arthritis
Surgery
Doctors usually recommend surgery only if nonsurgical treatments have failed. Surgery may be needed if the problem is caused by a bone abnormality. In the most common surgery for snapping scapula, the surgeon takes out a small piece of the upper corner of the scapula nearest to the spine.
Bone Resection
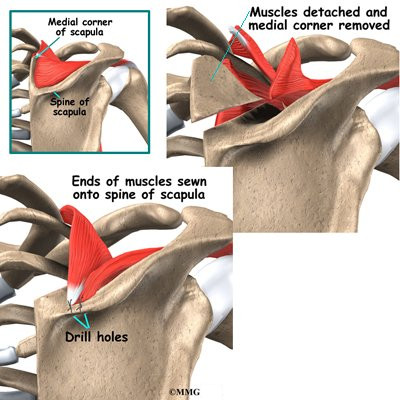
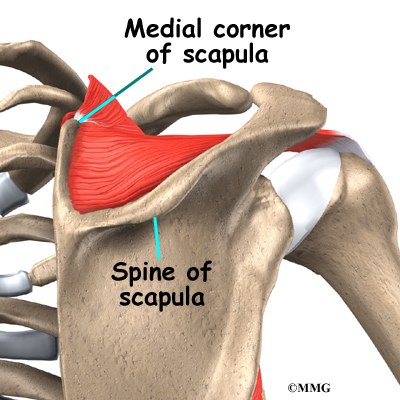
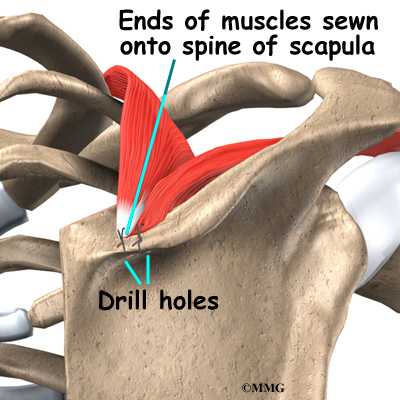
To remove a small piece of the scapula, an incision is made just below the bone’s top edge. The surgeon pulls aside the tissues to show the prominent section of the bone, called the spine of the scapula. The tissues that attach muscles to the upper part of the scapula are carefully detached and moved out of the way. Then the surgeon uses a special tool to remove the corner of the scapula. Drill holes are made into the spine of the scapula. Then the ends of the upper scapular muscles are sewn back onto the spine of the scapula, and the incision is closed up.

Arthroscopic Bursectomy
Surgeons sometimes do arthroscopic surgery to take out an inflamed scapulothoracic bursa. Removing a bursa is called bursectomy. Small incisions allow the surgeon to insert a small TV camera, called an arthroscope, into the joint. Through another small incision, the surgeon uses special instruments to remove the inflamed bursa while the arthroscope shows what is happening.
Rehabilitation
What can I expect after treatment?
Nonsurgical Rehabilitation
For patients undergoing nonsurgical treatment, physical or occupational therapy may be part of the rehabilitation plan. Your therapist may help treat your pain and inflammation. Therapists also evaluate posture to make sure the spine and shoulder bones are in their best alignment. A strengthening program to bulk up the muscles under the scapula may help pad and cushion the soft tissues between the scapula and rib cage.
After Surgery
Therapy is more involved after surgery. Patients wear a sling following scapula surgery. Passive shoulder movements can begin soon after surgery. But there should be no active exercises for about eight weeks, to make sure the muscles are firmly healed where they were sewn back into the drill holes in the scapula. People usually start doing resistive exercise and activities after 12 weeks. Your surgeon will probably recommend that you work with a physical or occupational therapist during your rehabilitation.